Inguinal hernias
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Laurence KnottLast updated 13 Jan 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Hernia article more useful, or one of our other health articles.
In this article:
Continue reading below
What is an inguinal hernia?
An inguinal hernia comprises a protrusion of abdominal contents through the fascia of the abdominal wall, through the internal inguinal ring. Hernias always contain a portion of peritoneal sac and may contain viscera, usually small bowel and omentum.
Inguinal hernia
Inguinal hernia epidemiology
Inguinal hernias comprise approximately 7% of all surgical outpatient visits1 .
Male:female ratio of groin hernias is 8:12 .
Hernias and hydroceles occur in 1-3% of full-term infants3 .
In men, the incidence rises from 11 per 10,000 person-years, aged 16-24 years, to 200 per 10,000 person-years, aged 75 years or above4 .
Risk factors
In infants: prematurity, male sex.
In adults: male sex, obesity, constipation, chronic cough, heavy lifting.
Continue reading below
Inguinal hernia presentation
Swelling in the groin that may appear with lifting and be accompanied by sudden pain.
Indirect hernias are more prone to cause pain in the scrotum and cause a 'dragging sensation'.
An impulse (increase in swelling) may be palpable on coughing.
It may not be possible to see the hernia if it is reduced.
If a lump is present, it may be reducible.
Congenital inguinal hernias are usually detected at birth and all need urgent outpatient referral for surgical repair.
Inguinal hernias in older children and adults usually develop gradually but can occur suddenly with an episode of heavy lifting causing 'rupture':
At first appearance, a hernia is usually easily reducible when the patient reclines. However, it may require manual replacement if large.
With time, the hernia enlarges and becomes harder to replace, due to fibrous adhesions forming.
When it can no longer be reduced, it is irreducible or incarcerated. This can occur at any time, as can strangulation. This occurs when visceral contents of the hernia become twisted or entrapped by the narrow opening. This compromises the blood supply, causing swelling and eventually infarction. Strangulation usually leads to bowel obstruction.
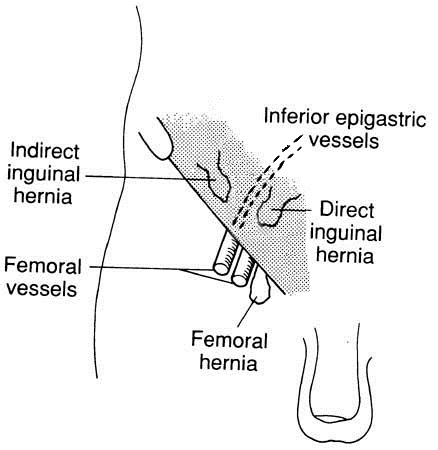
There are two types of inguinal hernia:
Indirect: a protrusion through the internal inguinal ring passes along the inguinal canal through the abdominal wall, running laterally to the inferior epigastric vessels. This is the more common form accounting for 80% of inguinal hernias, especially in children. It is associated with failure of the inguinal canal to close properly after passage of the testis in utero or during the neonatal period5 .
Direct: the hernia protrudes directly through a weakness in the posterior wall of the inguinal canal, running medially to the inferior epigastric vessels. It is more common in the elderly and rare in children.
The clinical findings will help suggest whether the inguinal hernia is direct or indirect; in adults this is usually confirmed at operation. There may be a limit to the clinical utility of such a distinction, especially in adults.
The less common form is the sliding hernia where a portion of viscera slides behind the peritoneal sac into the inguinal canal with the wall of the organ forming part of the hernial sac.
Assessment
Examine the patient both standing and lying and ask them to cough or strain.
Insert a finger through the top of the scrotum into the external inguinal ring and palpate for a lump when coughing - cough impulse.
Sliding hernias are probable with large scrotal hernias.
Differential diagnosis
See also the separate Lumps in the Groin and Scrotum article.
Femoral hernia: this is seen in various forms, at simplest as a small swelling in the top of the inside of the thigh. Alternatively, it may be deflected to appear higher as an inguinal hernia. It is either irreducible or reduces only slowly with pressure.
Hydrocele (when differentiating from an inguinoscrotal hernia, note that it is possible to get above a hydrocele on examination).
Spermatic cord hydrocele.
Lymph node swelling.
Abscess.
Saphena varix.
Bleeding.
Continue reading below
Investigations
Ultrasound is the less invasive method, if there is doubt. MRI or CT scanning may also be used5 6 . Herniography with injection of X-ray contrast agent into the peritoneum is rarely necessary7 .
Inguinal hernia treatment and management
Adults7
If the inguinal hernia is small, the patient may only need reassurance. However, there is always the chance of it becoming a surgical emergency through obstruction and incarceration. Episodes of pain and tenderness suggest the need for urgent treatment but when these become prolonged and severe then emergency surgery is indicated for possible strangulation. The fundamentals of indirect inguinal hernia treatment are the same regardless of the patient's age. Reduction or excision of the sac and closure of the defect with minimal tension are the essential steps in any hernia repair.
Conventional surgery was based on Bassini's operation; this consisted of apposition of the transversus abdominis and transversalis fascia and the lateral rectus sheath to the inguinal ligament. The Shouldice technique uses two layers of running suture in a similar fashion.
However, the Lichtenstein technique is widely used, where a piece of open-weave polypropylene mesh is used to repair and reinforce the abdominal wall. This operation is easier to learn, gives earlier mobility and has a very low recurrence rate. The standard repair now uses prostheses, usually polypropylene mesh.
Concerns that some of the traditional meshes were heavy and associated with postoperative stiffness and pain led to the development of lighter meshes. A systematic review failed to find any differences in long-term and short-term complications between the two8 . A subsequent meta-analysis concluded that heavyweight mesh had a distinctive advantage over lightweight mesh with regard to recurrence. The two types of prosthetic meshes had equivalent outcomes for postoperative pain, seroma, foreign body sensation, infection, and numbness9 .
Postoperative infection has been a concern when a mesh is used. However, antibiotic prophylaxis in average-risk patients in low-risk environments is not recommended in open surgery. In laparo-endoscopic repair it is never recommended.
Bilateral hernias are best repaired laparoscopically. There is less postoperative pain, full recovery is better and return to work is faster. However, the price is increased compared with the conventional approach and there appears to be a higher number of serious complications of visceral (especially bladder) and vascular injuries10 .
There are two approaches: either the transabdominal preperitoneal (TAPP) or the totally extraperitoneal (TEP) procedure. In TAPP, the surgeon goes into the peritoneal cavity and places a mesh through a peritoneal incision over possible hernia sites. TEP is different, as the peritoneal cavity is not entered and mesh is used to seal the hernia from outside the peritoneum. The mesh, where used, becomes incorporated by fibrous tissue.
Meta-analyses found that laparoscopic and open mesh repairs for recurrent inguinal hernias were equivalent in most of the analysed outcomes.
Preferences in surgical techniques vary across the world. In the USA and some parts of Europe, laparoscopic repair is becoming the first-line option for all types of hernias.
The British Hernia Society has not released guidelines since the International Guidelines were released, but comment in their advice to patients that laparoscopy may be beneficial for recurrent hernias, bilateral hernias, hernias in women, and very active patients in whom the predominant symptom is pain. Open repair under anaesthetic may be better in older patients with comorbidities or in those who do not want a full general anaesthetic11 .
Surgery can be performed on a day-case basis; for seven days afterwards the patient should avoid driving and lifting. The patient should be able to resume normal activities over the subsequent 2-3 weeks but, with a heavy job, it can take up to six weeks to return to work.
A truss may be required where surgery is inadvisable or refused; however, it can be difficult for patients to manage and cannot be recommended as a definitive form of treatment.
Inguinal hernias in children
The incidence of incarcerated or strangulated hernias in paediatric patients is 12-16%12 . 50% of these occur in infants aged younger than 6 months13 .
Paediatric surgeons will repair soon after diagnosis, regardless of age or weight, in healthy full-term infant boys with asymptomatic reducible inguinal hernias. There is no significant difference in operative time for unilateral hernias but laparoscopy is faster than open surgery for bilateral hernias. There is no difference in recurrence rate but wound infection is higher with open surgery than with laparoscopy14 .
The timing of inguinal hernia repair in premature infants remains a controversial topic. They are often repaired prior to discharge from the neonatal intensive care unit (NICU). However, since infants are now being discharged home at much lower weights there has been a trend towards postponing surgery for 1-2 months to allow further growth. One study advocated early surgery in order to avoid perioperative morbidity and to reduce the risk of incarceration, subsequent testicular ischemia and hernia recurrence15 . A systematic review concluded that repair of inguinal hernia in premature infants before NICU discharge may increase the odds of recurrence, but not incarceration or surgical complications16 .
Herniotomy is all that is required with ligation and excision of the patent processus vaginalis.
Complications
These include4 :
Recurrence: 1.0% - most happening within five years of operation. Recurrence rate increases:
In children aged younger than 1 year.
In elderly patients.
After incarcerations.
In those with ongoing increased intra-abdominal pressure.
Where there is growth failure.
With prematurity.
Where there are chronic respiratory problems.
In girls with sliding hernias.
Infarcted testis or ovary with atrophy.
Wound infection.
Bladder injury.
Intestinal injury.
A hydrocele from fluid accumulation in the distal sac usually resolves spontaneously but sometimes requires aspiration.
Prognosis
This is generally very good, depending on comorbidity.
Further reading and references
- Jorgenson E, Makki N, Shen L, et al; A genome-wide association study identifies four novel susceptibility loci underlying inguinal hernia. Nat Commun. 2015 Dec 21;6:10130. doi: 10.1038/ncomms10130.
- Gudigopuram SVR, Raguthu CC, Gajjela H, et al; Inguinal Hernia Mesh Repair: The Factors to Consider When Deciding Between Open Versus Laparoscopic Repair. Cureus. 2021 Nov 16;13(11):e19628. doi: 10.7759/cureus.19628. eCollection 2021 Nov.
- Seifmanesh H et al; Castleman’s disease in a patient with inguinal mass mimicking hernia. Am J Case Rep 2010; 11:211-213.
- Burcharth J, Pedersen M, Bisgaard T, et al; Nationwide prevalence of groin hernia repair. PLoS One. 2013;8(1):e54367. doi: 10.1371/journal.pone.0054367. Epub 2013 Jan 14.
- Docimo S; The Kelalis-King-Belman Textbook of Clinical Pediatric Urology, Fifth Edition, 2006.
- Jenkins JT, O'Dwyer PJ; Inguinal hernias. BMJ. 2008 Feb 2;336(7638):269-72.
- Burkhardt J et al; Diagnosis of Inguinal Region Hernias with Axial CT: The Lateral Crescent Sign and Other Key Findings, 2010.
- LeBlanc KE, LeBlanc LL, LeBlanc KA; Inguinal hernias: diagnosis and management. Am Fam Physician. 2013 Jun 15;87(12):844-8.
- HerniaSurge Group; International guidelines for groin hernia management. Hernia. 2018;22(1):1-165. doi:10.1007/s10029-017-1668-x
- Currie A, Andrew H, Tonsi A, et al; Lightweight versus heavyweight mesh in laparoscopic inguinal hernia repair: a meta-analysis. Surg Endosc. 2012 Aug;26(8):2126-33. doi: 10.1007/s00464-012-2179-6. Epub 2012 Feb 7.
- Wu F, Zhang X, Liu Y, et al; Lightweight mesh versus heavyweight mesh for laparo-endoscopic inguinal hernia repair: a systematic review and meta-analysis. Hernia. 2020 Feb;24(1):31-39. doi: 10.1007/s10029-019-02016-5. Epub 2019 Jul 31.
- McCormack K, Scott NW, Go PMNYH, Ross S, Grant AM, the EU Hernia Trialists Collaboration; Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database of Systematic Reviews 2000, Issue 4. Art. No. CD001785. DOI: 10.1002/14651858.CD001785
- Groin Hernia and You; British Hernia Society, 2022
- Lawal TA, Egbuchulem KI, Ajao AE; Obstructed inguinal hernia in children: case-controlled approach to evaluate the influence of socio-demographic variables. J West Afr Coll Surg. 2014 Apr-Jun;4(2):76-85.
- Nigam V; Essentials of Abdominal Wall Hernias, 2009.
- Esposito C, St Peter SD, Escolino M, et al; Laparoscopic versus open inguinal hernia repair in pediatric patients: a systematic review. J Laparoendosc Adv Surg Tech A. 2014 Nov;24(11):811-8. doi: 10.1089/lap.2014.0194. Epub 2014 Oct 9.
- Vaos G, Gardikis S, Kambouri K, et al; Optimal timing for repair of an inguinal hernia in premature infants. Pediatr Surg Int. 2010 Apr;26(4):379-85. doi: 10.1007/s00383-010-2573-x. Epub 2010 Feb 19.
- Masoudian P, Sullivan KJ, Mohamed H, et al; Optimal timing for inguinal hernia repair in premature infants: a systematic review and meta-analysis. J Pediatr Surg. 2019 Aug;54(8):1539-1545. doi: 10.1016/j.jpedsurg.2018.11.002. Epub 2018 Nov 14.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 12 Jan 2027
13 Jan 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free