Pre-operative assessment - examination and tests
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Laurence KnottLast updated 22 Feb 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article:
Continue reading below
What is a pre-operative assessment?
Every year more than three million operations are performed. It is common practice to perform a pre-op (operation) assessment on patients before they go to theatre. Commonly used investigations are discussed below. (A careful history should have been taken initially in order for as much information to be obtained as possible from the patient before any examination or investigations occur.)
Examination
General
A general systems examination should identify obvious abnormalities:
Cardiovascular system - heart murmur. With the exception of emergency surgery, patients should be haemodynamically stable and their vital signs normal before starting anaesthesia.
Respiratory system - abnormal breath sounds.
Gastrointestinal system - abdominal masses, previous scars.
Musculoskeletal system - skeletal malformations such as kyphoscoliosis.
General - local skin infection.
Airway assessment
How easy or difficult it will be to intubate a patient depends on the following points:
Are they obese?
Do they have a short neck and small mouth?
To what extent can they open their mouth?
Is there any soft tissue swelling at the back of the mouth or are there any limitations in neck flexion or extension?
Continue reading below
Investigations
The doctor should ask whether the result of the test is going to alter the patient's management. Ordering unnecessary tests is neither helpful nor cost-effective.
Following reviews on the available evidence of the value of routine pre-op assessments in healthy or asymptomatic adults, the National Institute for Health and Care Excellence (NICE) produced guidance on the subject1 . A pre-op assessment covers tests that are often carried out when a patient is scheduled for elective surgery. Pre-op assessments may be performed by a variety of health professionals, in different settings. Pre-op assessments make recommendations on the circumstances in which the tests should be done, not done, or considered. Whether a certain test is recommended may depend on the patient's risk factors, or how serious the planned operation is.
Online tools also exist which will recommend which pre-operative assessments are necessary for an individual patient, based on age, comorbidities and type of procedure scheduled (see under Further Reading and References, below).
FBC
This will demonstrate anaemia. This increases the risk of intra-operative hypoxia or increased cardiac workload. There is also an increased risk of myocardial infarction or cerebrovascular event and delayed healing. It is also useful as a baseline measure of haemoglobin if the proposed operation is expected to cause substantial blood loss.
U&Es
This detects underlying renal deficiency and the possibility of developing acute kidney failure after major surgery. It may also influence the choice of drugs given within the anaesthetic.
LFTs
Does the patient have any underlying malnutrition? This may affect the patient's ability to heal. Is there a clotting problem?
Calcium
Is there a suggestion of underlying malignancy? Abnormal calcium levels can impact on heart rhythm and so may need to be corrected prior to any surgery.
Clotting
Clotting and platelet function is relevant for the many patients who take aspirin or warfarin; also, for patients with known clotting disorders, or in those with altered LFTs for any reason.
Group and save (or hold)
Anticipating that there may be a requirement for blood but not routinely for this procedure, the patient's blood type is identified and held, pending a possible (later) request for units of blood or blood products.
Cross-match
A requirement for transfusion needs to be anticipated to avoid high demand/unavailable resource. The surgeon makes a prediction (in units of blood) for the procedure. That amount, typed specifically for that patient, is held in the blood bank for 24 hours. The decision about whether to cross-match serum or to order group and save should be judged on the current haematological status of the patient as well as the estimated blood loss.
Urinalysis
Urine dipstick or analysis is useful to detect undiagnosed diabetes or urinary tract infection. It may also detect haematuria or abnormal protein loss.
CXR
If unselected, CXR may contribute litte to patient management in routine surgery2 . Royal College of Radiology guidelines (available as an online tool, for purchase - 'iRefer') give clear indications for CXR pre-operatively3 .
Those with suspected metastases.
Those with possible or established cardio-respiratory disease, who have not had a chest radiograph within the last 12 months.
Recent immigrants from countries where tuberculosis is still endemic and who have not had a chest radiograph within the last 12 months.
Those with a recent history of chest trauma.
Those whose surgery may involve a thoracotomy.
Those undergoing major abdominal surgery, where respiratory complications are a possibility.
Heavy smokers who have not had a chest radiograph within the last 12 months.
Patients not included in the above categories, if the request is made by the appropriate anaesthetist.
A CXR should only be requested by the anaesthetist for assessment, or if they felt the patient may need admission to ITU postoperatively2 .
Thyroidectomy or head and neck surgery.
Neurosurgery - because of prolonged nature of anaesthesia and need for postoperative ITU
Lymph node surgery.
Spirometry
Spirometry tests are a good measure of pulmonary physiology and are useful in patients with obstructive or restrictive patterns of disease.
ECG
NICE recommends that1 :
ECG should not be performed routinely for patients undergoing minor surgery but should be considered for those who have not had one within the preceding 12 months. It will show any silent myocardial ischaemia or infarction, will provide a baseline for any future postoperative events, and may detect arrhythmia.
For intermediate surgery, routine ECG is not necessary, but should be considered for patients with cardiovascular, renal or diabetes comorbidities.
For major surgery, ECG should be considered for people aged over 65 if no results are available from the past 12 months.
Sickle cell testing
It is important to offer testing pre-operatively to identify risk before the anaesthetic - surgical or dental. This is important for ethnic groups who have a family history of homozygous sickle cell anaemia or sickle cell trait, particularly where there is no previous surgical history.
At-risk groups include:
African
Caribbean
Eastern Mediterranean
Middle Eastern
Asian
It has also been found in Cypriot people.
Appropriate counselling is important, so that the patient realises the implication of both positive and negative results and is able to give informed consent.
Pregnancy testing
The need to test depends on the risk to the fetus from the surgery and anaesthetic. These risks should be explained to the patient.
The woman should be asked sensitively if there is any possibility of pregnancy. If there is any doubt, a test should be done with the woman's consent. Similar questioning should be carried out before a CXR.
Pre-operative assessment
The American Society of Anesthesiologists' (ASA) grades for adults4
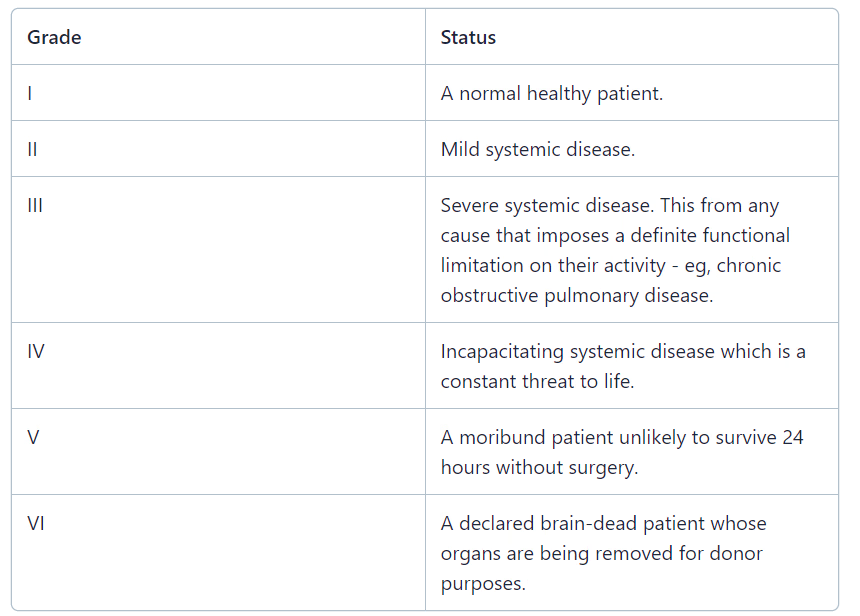
Recommendations on which pre-op assessments are necessary are based on ASA grade and level of surgery or specialty; there are special recommendations for neurosurgery and cardiac surgery. Any comorbidity (eg, cardiovascular, respiratory or renal) are also taken into account.
For example, grade 1 surgery:
Continue reading below
Grading of surgical procedures by severity - examples1
Minor
Excising skin lesion.
Draining breast abscess.
Intermediate
Primary repair of inguinal hernia.
Excising varicose veins in the leg.
Tonsillectomy or adenotonsillectomy.
Knee arthroscopy.
Major or complex
Total abdominal hysterectomy.
Endoscopic resection of prostate.
Lumbar discectomy.
Thyroidectomy.
Total joint replacement.
Lung operations.
Colonic resection.
Radical neck dissection.
Further reading and references
- Consent guidance: patients and doctors making decisions together; General Medical Council, Sep 2020
- Bader AM; Advances in preoperative risk assessment and management. Curr Probl Surg. 2012 Jan;49(1):11-40.
- 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management; European Society of Cardiology (Aug 2014)
- National Guideline Centre (UK); Evidence review for preoperative risk stratification tools: Perioperative care in adults: Evidence review C. London: National Institute for Health and Care Excellence (NICE); 2020 Aug. (NICE Guideline, No. 180.)
- Routine preoperative tests for elective surgery; NICE Guidelines (April 2016)
- Joo HS, Wong J, Naik VN, et al; The value of screening preoperative chest x-rays: a systematic review. Can J Anaesth. 2005 Jun-Jul;52(6):568-74.
- Duncan K et al; Preoperative CXR prior to elective surgery, Royal College of Radiologists, 2008
- ASA Physical Status Classification System; American Society of Anesthesiologists
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 21 Feb 2027
22 Feb 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free