Haemophilia
Peer reviewed by Dr Krishna Vakharia, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 31 Mar 2023
Meets Patient’s editorial guidelines
Haemophilia is a rare bleeding disorder that affects your ability to make a clot. The blood contains substances called clotting factors that work with platelets to form a clot. When you injure yourself the clot stops you bleeding. Haemophilia is a condition where there is a deficiency of clotting factors, so people with this condition usually have prolonged bleeding. There is no cure but with available treatments most people with haemophilia are able to live normal lives.
In this article:
Continue reading below
What is haemophilia?
Haemophilia is a rare bleeding disorder caused by deficiency of clotting factors. Clotting factors are present in the blood and are responsible for forming blood clots in response to an injury. Haemophilia B is the more common problem and is due to a deficiency of clotting factor IX. Haemophilia A is due to a deficiency of clotting factor VIII. By and large, haemophilia B tends to be less severe than haemophilia A but they are similar.
The vast majority of cases are inherited, so people are usually born with the condition.
Both haemophilias are inherited as X-linked recessive conditions. This describes how the abnormal haemophilia gene is passed from parent to child.
Genes and haemophilia
In the centre (nucleus) of most cells in your body, the DNA molecule is packaged into thread-like structures called chromosomes. You have 46 chromosomes arranged in 23 pairs. These include one pair of sex chromosomes (either XX for females or XY for males). The other chromosomes that do not determine whether we are male or female are called autosomes. There are 22 pairs of autosomes (numbered 1 to 22). One chromosome from each pair comes from your mother and one from your father.
A gene is the basic unit of your genetic material. It is made up of a sequence (or piece) of DNA and sits at a particular place on a chromosome. So, a gene is a small section of a chromosome. Each gene controls a particular feature or has a particular function in your body. For example, dictating your eye or hair colour, or making all the various proteins in your body, such as clotting factors. Each gene is part of a pair. One gene from each pair is inherited from your mother, the other from your father. The genes have been copied from the parents' cells into the child's cells.
Genes are found on 'chromosomes', rather like houses on a street. The gene causing haemophilia is located on a chromosome called the X chromosome. Boys have one X chromosome and one Y chromosome; girls have two X chromosomes.
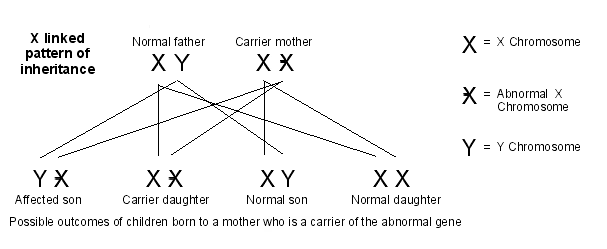
X-linked inheritance pattern
Haemophilia is inherited in a pattern called 'X-linked recessive inheritance'. The haemophilia gene is 'carried' by women but does not usually cause problems in girls or women (with rare exceptions). This is because of there being two X chromosomes in women: one X chromosome has the 'faulty' gene; the other X chromosome has a normal gene, which compensates for the faulty one. The 'recessive' means that the effects of a 'faulty' X gene can be masked by a normal gene being present.
Males with the haemophilia gene do not have a second X chromosome and so they cannot compensate for the faulty gene. Therefore, boys with the haemophilia gene always have symptoms of the disease.
The haemophilia gene can be passed on from parent to child. For a woman who carries the gene, there is a 1 in 2 chance that her sons will have haemophilia, and a 1 in 2 chance that her daughters will carry the gene.
X-linked inheritance pattern
Continue reading below
What causes haemophilia?
The abnormal gene (that is inherited in haemophilia) causes a deficiency of a clotting factor. A lower level of clotting factor means you do not form a clot as quickly as other people. The deficiency does not stop you from clotting completely asthere are some clotting factors remaining, but the lower the amount of clotting factors, the more serious the disease will be.
Haemophilia A happens in around 1 in 4-5,000 live male births per year. Haemophilia B occurs in around 1 in 30,000 live births. No country seems to escape the condition and neither is any country particularly prone to it.
You can, rarely, acquire haemophilia after birth. This happens largely in older patients, due to the immune system attacking clotting factors or because of blood cancers (haematological malignancies). Sometimes spontaneous mutations happen in the genes of families from certain geographical areas, such as Sweden.
Gender (sex) differences in haemophilia
Because haemophilia is inherited in an X-linked recessive pattern, male babies are usually affected. Their mothers carry the gene but are not affected.
There is usually a clear family history but random cases do occur due to gene changes such as spontaneous mutations. Females born to affected fathers can (rarely) have the disease depending on how their genes are made up. Sometimes this might occur, for instance, where there is marriage to close relatives in the family.
Haemophilia symptoms
Signs and symptoms of haemophilia are different according to the severity of the condition.
Severe disease
Neonatal bleeding may follow any surgery, such as circumcision. Internal bleeding in the skull can be a feature of severe cases as can a large bruise (haematoma) and prolonged bleeding from the cord or umbilical area.
History of spontaneous bleeding into the joints, especially the knees, ankles and elbows, without a history of significant trauma.
Bleeding into muscles may also occur.
Bleeding into the gut can occur but is more often associated with haemophilia B.
Blood in the urine (haematuria) may be a feature, but it can vary in amount.
Untreated cases of severe disease
This group of patients may develop the following:
Joint problems and deformity - they may need joint replacement.
Spontaneous bleeding into soft tissues is common. This may cause complications such as compartment syndrome.
Bruise (haematoma) formation - may happen spontaneously or following trauma and may need surgical removal if very large.
Moderate disease
Often presents with bleeding following blood tests (venepuncture).
Mild disease
People with this only have prolonged bleeding after major trauma or surgery.
Continue reading below
Haemophilia diagnosis
Blood tests are used to diagnose haemophilia and to find out how severe it is. If there's no family history of haemophilia, it's usually diagnosed when a child begins to walk or crawl. At this time it might be noticed that the child is bruising very easily, or having very large bruises.
Mild haemophilia may only be discovered later, usually after an injury or following a dental or a surgical procedure.
Diagnosis during pregnancy
If you have a family history of haemophilia and you're planning to get pregnant, genetic testing can help you find out the risk of passing the condition on to a child.
This may involve testing a sample of your blood to look for signs of the genetic change that causes haemophilia.
There are tests that can diagnose haemophilia in the baby when you are pregnant. They include:
Chorionic villus sampling (CVS) - a small sample of the placenta is removed from the womb and tested for the haemophilia gene, usually during weeks 11 to 14 of pregnancy.
Amniocentesis - a sample of amniotic fluid is taken for testing, usually during weeks 15 to 20 of pregnancy.
There's a small risk of these procedures causing problems such as miscarriage or premature labour. This can be worrying so you may find it helpful to discuss this with your doctor.
If haemophilia is suspected after the baby is born, blood tests on the child can usually confirm the diagnosis. Blood from the umbilical cord can be tested at birth.
Haemophilia treatment
Currently there is no cure for haemophilia, but the available treatments can allow a good quality of life.
Artificial (man-made) clotting factors are given as medicines to prevent, or to treat, prolonged episodes of bleeding. These medicines are given as an injection and are the mainstay of treatment in the UK.
If you have a fairly good level of clotting factors (mild symptoms), injections are usually only given if you have an extended bleed. More severe cases are treated with regular injections to prevent prolonged bleeding.
A newer treatment has been developed that does not directly replace the clotting factor. It is a monoclonal antibody - a medicine that mimics factor VIII - called emicizumab that is an option for haemophilia A. It allows the clotting cascade to happen, even without factor VIII.
Living with haemophilia
The majority of people with haemophilia can live a normal life. There are some general rules you should try to keep to and remember:
Avoid contact sports, such as rugby.
Consider alternatives to shaving - grow a beard.
You are allowed to donate blood if you are a carrier, but not if you have haemophilia.
Ask advice from your specialist if you are considering a tattoo or piercing.
You are NOT entitled to free prescriptions because you have haemophilia.
Take care with other medicines that can affect your ability to clot. Your healthcare professional will bear this in mind when prescribing but some are available over the counter, such as aspirin and ibuprofen.
Have regular check-ups at the dentist to ensure your teeth and gums are healthy.
Looking after your teeth and gums helps you avoid problems such as gum disease, which can cause bleeding. Most non-surgical dental treatment can be done at a normal dental surgery.
People with haemophilia are cared for by a hospital haematology department and they can give you advice about dental care, and further information and advice about living with haemophilia.
If you have haemophilia, you should also register at your local haemophilia centre. It's a useful source of advice and support.
Further reading and references
- The Haemophilia Society
- Mazzucconi MG, Baldacci E, Ferretti A, et al; Acquired Haemophilia A: An Intriguing Disease. Mediterr J Hematol Infect Dis. 2020 Jul 1;12(1):e2020045. doi: 10.4084/MJHID.2020.045. eCollection 2020.
- Aledort L, Mannucci PM, Schramm W, et al; Factor VIII replacement is still the standard of care in haemophilia A. Blood Transfus. 2019 Nov;17(6):479-486. doi: 10.2450/2019.0211-19. Epub 2019 Dec 11.
- Guidelines for the use of prophylactic factor replacement for children and adults with Haemophilia A and B; British Society for Haematology (May 2020)
- Mahlangu J, Iorio A, Kenet G; Emicizumab state-of-the-art update. Haemophilia. 2022 May;28 Suppl 4(Suppl 4):103-110. doi: 10.1111/hae.14524.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 29 Mar 2028
31 Mar 2023 | Latest version
31 Mar 2023 | Originally published
Authored by:
Dr Hayley Willacy, FRCGP

Feeling unwell?
Assess your symptoms online for free