Hand, foot and mouth disease
Peer reviewed by Dr Laurence KnottLast updated by Dr Colin Tidy, MRCGPLast updated 20 Oct 2021
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Hand, foot and mouth disease article more useful, or one of our other health articles.
In this article:
Continue reading below
What is hand, foot and mouth disease?
Hand, foot and mouth disease (HFMD) is a viral illness which commonly causes lesions involving the mouth, hands and feet. However, it may also affect other areas such as the buttocks and genitalia. The most common causes of hand, foot and mouth disease are Coxsackievirus A16 (CA16) and enterovirus 71 (EV71). It is normally a mild, self-limiting illness but occasionally has serious complications, and fatalities have occurred in epidemics around the world.
Epidemiology1 2
Hand, foot and mouth disease occurs worldwide, with a peak incidence in the summer and autumn in temperate climates.
It typically affects children younger than 10 years of age, especially children younger than 4 years of age.
Outbreaks occur frequently in nurseries, childcare centres, and schools. Spread within families is also common.
Most adults are immune following previous exposure. However, adult cases may occur, especially with Coxsackievirus A6 infection..
Epidemics have occurred in Southeast Asia in particular in recent years. A large outbreak occurred in China in 2009, with numbers of fatalities above 300. China has led the development of a vaccine. Those caused by enterovirus 71 are more likely to cause neurological complications and fatalities; however, CA16 has also been involved in epidemics and deaths3 .
Continue reading below
Hand, foot and mouth disease causes1
Hand, foot and mouth disease is most often caused by the group A Coxsackieviruses (particularly CA16) or enterovirus 71 (EV71). These closely related viruses are of the Picornaviridae family, Enterovirus genus which includes echoviruses and polioviruses. It can be caused by other group A and B Coxsackieviruses, particularly Coxsackieviruses A6 and A104 5 .
Transmission is commonly by the faecal-oral route. Contact with skin lesions and oral secretions (including coughs and sneezes) can also allow transmission. An infected individual can continue to shed the virus in the stools for some weeks.
The incubation period is 3-7 days.
Hand, foot and mouth disease symptoms1
The mucocutaneous lesions appear 1-2 days after a prodromal period of fever, malaise and myalgia; and last approximately 7-10 days with spontaneous resolution.
Prodrome: includes a low-grade fever, malaise and loss of appetite. There may be a sore mouth or throat, cough or abdominal pain. EV71 can occasionally cause vomiting.
Diagram illustrating mouth, hand and foot lesions
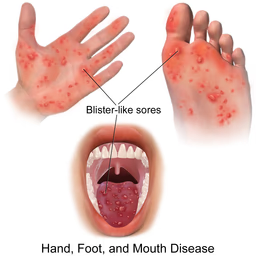
By BruceBlaus, CC BY-SA 4.0, via Wikimedia Commons
Mouth lesions: after the prodrome, lesions develop in the mouth. These may be on the buccal mucosa, tongue and hard palate. The uvula, gums, lips and skin around the mouth are sometimes involved. They begin as macular lesions that progress to vesicles which then erode. Mouth lesions are typically yellow ulcers surrounded by red haloes. They may be uncomfortable or painful. Children aged less than 5 years tend to have more severe symptoms than older children.
Skin lesions: most usually then also develop skin lesions. They are mainly on the palms, soles and between the fingers and toes. Lesions start as 2-5 mm erythematous macules but rapidly progress to grey vesicles with an erythematous base. Lesions may also appear on the trunk, thighs, buttocks and/or genitalia. These less typical lesions are mainly an erythematous maculopapular rash rather than the papulovesicular ones found on the hands and feet. The rash lasts about 3-6 days. Lesions are usually asymptomatic but can be itchy or painful.
Continue reading below
Differential diagnosis1
Herpangina (caused by similar Coxsackieviruses or echoviruses with lesions similar to hand, foot and mouth disease but limited to the posterior oral cavity with no skin lesions).
Viral pharyngitis.
Oral forms of lichen planus.
Investigations1 2
Diagnosis is usually clinical and investigations are not usually necessary.
The virus can be isolated from throat, vesicle or rectal swabs (placed in viral transport medium) or from faecal culture. Viral shedding in faeces can be intermittent so more than one specimen may be required.
Polymerase chain reaction (PCR) has made enteroviral subtyping possible and is increasingly the test of choice in specialist centres, although rarely used in routine clinical practice.
Hand, foot and mouth disease treatment1
There is no known treatment, so management is generally supportive:
Parents may need to be reassured that it is unrelated to foot and mouth disease in animals.
Encourage adequate fluid intake. If the mouth is uncomfortable, dehydration may result from poor fluid intake.
Suggest a soft diet (soup, ice cream, mashed potato, etc).
Antipyretic analgesics, such as paracetamol or ibuprofen, are usually all that is required.
If the mouth is very painful, the following topical agents can be considered although there is no evidence of efficacy:
Lidocaine oral gel.
Benzydamine spray or mouth wash. (Spray only for those aged over 5 years, mouthwash for those aged over 12 years.)
Choline salicylate oral gel (not advised in children under the age of 16 years or in women who are pregnant or breastfeeding).
Mouth rinses with warm salty solutions if the person can be relied upon not to swallow it.
Any cardiovascular or neurological complications need to be treated appropriately in secondary care (see below).
Indications to consider referral
Signs of significant dehydration (particularly in a child). Admission to hospital is rarely required.
Neurological signs or symptoms - eg, myoclonic jerks, persistent or severe headaches, signs of developing encephalitis.
Persistent oral ulcers.
Advice about school and childcare settings
Public Health England does not recommend that children be kept away from school/nursery/childcare for any period of time6 . There is no need to isolate a child with HFMD and it is not notifiable.
Advise on general hygiene measures (see 'Prevention', below).
Advice for pregnant women
There are no known adverse consequences for the fetus if a pregnant woman is in contact with HFMD. Seek specialist advice if a woman develops HFMD within three weeks of expected delivery, as there may be a risk of passing the infection to the newborn. In rare cases this can lead to severe infection in the neonate, although usually illness is mild.
Complications1 2
Complications are rare. They include the following:
Secondary infection of skin that has been scratched.
Painful stomatitis due to oral involvement. This can lead to dehydration.
Neurological involvement and meningitis are more likely if EV71 is the causative organism7 . Neurological involvement can include aseptic meningitis, encephalitis, neurogenic pulmonary oedema and acute flaccid paralysis. Tremors, ataxia and cranial nerve palsies can occur.
Cardiorespiratory failure can occur in severe cases.
Prognosis1
This is generally excellent with a full recovery in the vast majority people.
Symptoms tend to improve within 3-6 days, usually with full resolution of skin and mouth lesions within 7-10 days.
Those cases caused by EV17 have a greater likelihood of developing neurological complications, although this is rare. Aseptic meningitis usually resolves without sequelae but encephalitis is more likely to have adverse outcomes. During epidemics, particularly in the Western Pacific region, there have been a number of fatalities, particularly in the outbreak in China in 2009.
Infection results in immunity to the specific causative virus, but recurrence can occur with a different member of the enterovirus group.
Hand, foot and mouth disease prevention1
Good hygiene measures prevent spread within the family:
Thorough handwashing after using the toilet. There is evidence that handwashing has a significant protective effect8 .
Covering of nose and mouth when coughing or sneezing.
Hygienic disposal of used tissues and nappies.
Avoidance of sharing of cups, eating utensils, towels, etc.
The virus can be shed in faeces for some time after recovery, so good hygiene should be maintained.
China has led the way with development of, and clinical trials for, a vaccine to protect against hand, foot and mouth disease. Plans for an immunisation strategy against the more potentially fatal EV71 are underway in China9 10 . There is currently no vaccine against the Coxsackieviruses, although there is work being done in this area3 .
Further reading and references
- Hand foot and mouth disease; DermNet NZ
- Hand, foot and mouth disease; NICE CKS, August 2020 (UK access only)
- A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD); World Health Organization, 2011
- Mao Q, Wang Y, Yao X, et al; Coxsackievirus A16: epidemiology, diagnosis, and vaccine. Hum Vaccin Immunother. 2014;10(2):360-7. doi: 10.4161/hv.27087. Epub 2013 Nov 14.
- Kimmis BD, Downing C, Tyring S; Hand-foot-and-mouth disease caused by coxsackievirus A6 on the rise. Cutis. 2018 Nov;102(5):353-356.
- Downing C, Ramirez-Fort MK, Doan HQ, et al; Coxsackievirus A6 associated hand, foot and mouth disease in adults: clinical presentation and review of the literature. J Clin Virol. 2014 Aug;60(4):381-6. doi: 10.1016/j.jcv.2014.04.023. Epub 2014 May 9.
- Guidance on infection control in schools and other childcare settings; UK Health Security Agency (September 2017 - last updated February 2023)
- Choi CS, Choi YJ, Choi UY, et al; Clinical manifestations of CNS infections caused by enterovirus type 71. Korean J Pediatr. 2011 Jan;54(1):11-6. Epub 2011 Jan 31.
- Ruan F, Yang T, Ma H, et al; Risk Factors for Hand, Foot, and Mouth Disease and Herpangina and the Preventive effect of hand-washing. Pediatrics. 2011 Apr;127(4):e898-904. Epub 2011 Mar 21.
- Li L, Yin H, An Z, et al; Considerations for developing an immunization strategy with enterovirus 71 vaccine. Vaccine. 2015 Feb 25;33(9):1107-12. doi: 10.1016/j.vaccine.2014.10.081. Epub 2014 Nov 8.
- Liang Z, Wang J; EV71 vaccine, an invaluable gift for children. Clin Transl Immunology. 2014 Oct 31;3(10):e28. doi: 10.1038/cti.2014.24. eCollection 2014 Oct.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 19 Oct 2026
20 Oct 2021 | Latest version

Feeling unwell?
Assess your symptoms online for free