Tapeworms
Cestodes
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Colin Tidy, MRCGPLast updated 14 Jun 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Worm medicines article more useful, or one of our other health articles.
In this article:
Cestodes are tapeworms. There is a large variety of tapeworms but only those that are pathogenic to humans will be discussed here.
Continue reading below
Tapeworms that are pathogenic to humans
These include:
Taenia solium (pork tapeworm).
Taenia saginata (beef tapeworm).
Diphyllobothrium latum (fish or broad tapeworm).
Hymenolepis nana and Hymenolepis diminuta (dwarf tapeworm and rat tapeworm respectively).
Echinococcus granulosus and Echinococcus multilocularis (cause hydatid disease).
Spirometra spp. plerocercoid tapeworm larvae (resulting in sparganosis).
Taenia solium and Taenia saginata
These cause 'taeniasis'.
Epidemiology
Present worldwide.
Incidence is higher in developing countries - 10% of the population can be affected.
The pork tapeworm has a higher incidence.
Morphology
T. saginata
Adult T. saginata tapeworm
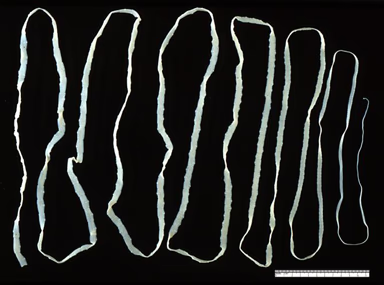
By CDC, Public Domain, via Wikimedia Commons
Usually less than 5 m long but can grow up to 25 m; 12 mm broad.
The head, called the scolex, is pear-shaped.
It has no hooks and no neck.
It has four suckers in the head.
The body is long and flat with several hundred segments called proglottids - hermaphroditic, egg-producing sections.
Each proglottid is 18 x 6 mm with a branched uterus.
Eggs are round and yellow-brown in colour.
T. solium
It has a variable size and can be up to 7 m long; it has a neck and a long flat body.
The scolex is globular in shape.
There are four suckers and hooks.
Proglottids are 5 x 10 mm and also have branched uteri.
Life cycle
Poorly cooked meat is ingested by humans who are the only definitive hosts. The poorly cooked meat includes tapeworm larval cysts (cysticerci) which then release larvae. These attach to the small intestine by the scolex suckers. The tapeworm then matures over 3-4 months during which the proglottids develop. The tapeworm can survive for up to 25 years in humans during which time the gravid proglottids are released into the faeces.
The excreted tapeworm eggs which are excreted in the faeces can survive on vegetation where they are then consumed by cattle or pigs. Once in these animals the eggs hatch and cysticerci are released. These pass into the animal circulation from the small intestine and reside in the muscle. Humans are then infected by eating raw meat containing the cysticerci.
Presentation
Taeniasis
This results from either T. saginata or T. solium and relates to the adult tapeworm in the gut.
This depends on the load of the infectious agents.
Light infection may be asymptomatic. Heavier infection leads to epigastric pain, diarrhoea and vomiting.
Cysticercosis
T. solium can also lead to cysticercosis whereby larval cysts infiltrate the lung, liver, eye or brain. This results in inflammation leading to clinical features such as severe sight impairment and neurological symptoms. In some countries (eg, Peru and Mexico) neurocysticercosis accounts for 30% of seizures,1 making it an important cause of morbidity and mortality worldwide.
Investigations
Recover eggs or proglottids in stool or perianal area.
Cysticercosis is confirmed by the presence of antibodies and imaging - eg, CXR, CT scan of the brain.
Treatment and management
Niclosamide or praziquantel (single dose) can be used (available on a named-patient basis).2
Treatment is very effective.3 Satisfactory treatment requires expulsion of the scolex.
There has been suggestion to use a purgative before and after to improve expulsion of the tapeworm.4
Prevention
Inspect meat thoroughly.
Adequate handling of food - eg, freezing or cooking.
Cysticerci do not survive temperatures of <10°C and >50°C.
The World Health Organization (WHO) advocates the periodic treatment of tapeworms such as T. solium in endemic areas with albendazole. This can prevent neurocysticercosis at a later stage.1
Continue reading below
Diphyllobothrium latum (fish or broad tapeworm)
Tapeworm infection results from eating raw or improperly cooked freshwater fish.
Epidemiology
Present worldwide, especially in subarctic and temperate regions.
Morphology
This is the longest tapeworm in humans - 3-10 m in length.
It has >3,000 proglottids which are more broad than long.
The scolex is shaped as two almond leaves.
Eggs are 35-55 x 55-75 micrometres.
Life cycle
Man and some animals are infected by this tapeworm. The plerocercoid larvae result in infection in humans. The cycle begins by the ingestion of uncooked fish containing plerocercoid larvae which attach to the small intestine. In 3-5 weeks the tapeworm matures to adult size. The adult tapeworm releases eggs that are passed into the faeces. These eggs hatch in fresh water, releasing ciliated coracidia. These are subsequently ingested by the water flea (cyclops) and release procercoid larvae. The cyclops are then ingested by freshwater fish, forming plerocercoid larvae which when ingested lead to infection.
Fish tapeworm symptoms
This depends on the number of tapeworms. Mild infection leads to:
Abdominal discomfort.
Loss of appetite.
Loss of weight.
Malnutrition.
B12 deficiency, which may occur with heavier infections and may lead to anaemia and even subacute combined degeneration of the spinal cord.
Investigations
Recover typical eggs or proglottids in stools.
Treatment and management
Praziquantel is first-line. Niclosamide can also be used.5
Prevention
Freeze fish for 24 hours.
Thoroughly cook fish.
Pickle fish.
Prevent sewage contamination of fish reservoirs.
Hymenolepis nana (dwarf tapeworm)
This is a relatively small tapeworm (15-40 mm) and tends to infect children. The reservoir is rodents and transmission is oro-faecal. Thus, cross infection and auto-infection are common in children.
Life cycle
The eggs are ingested and invade the small intestine where they mature into adult tapeworms. These adults reside for several weeks.
Dwarf tapeworm symptoms
Light infection is associated with vague abdominal pain but enteritis can occur with heavier infections.
Investigations
Presence of eggs in faeces.
Treatment and management
Niclosamide or a single dose of praziquantel are the drugs of choice.
Prevention
Good hygiene can effectively prevent spread.
Hymenolepis diminuta is the rat tapeworm. It is much longer than H. nana and primarily affects rats but very rarely it can be accidentally ingested by humans - eg, by ingestion of insects that carry the parasite. Most interest in it relates to research. The presentation and management are similar to those of H. nana.
Continue reading below
Echinococcus granulosus and Echinococcus multilocularis6 7
E. granulosus and E. multilocularis cause hydatid disease. Dogs and other canids are the definitive hosts.
E. granulosus
Epidemiology
E. granulosus is common in Asia, Australia, East Africa, southern regions of Spain, South America and North America. In these areas, 1-2 per 1,000 population are affected. Incidence rates are higher in some rural areas.
Morphology
E. granulosus is the smallest of the tapeworms (3-9 mm long) and it only has three proglottids.
Life cycle
The adult tapeworms live in domestic and in wild carnivorous animals. Infected animals pass eggs in their faeces, which are then ingested by grazing farm animals and humans. The eggs then localise in various organs, resulting in a hydatid cyst which contains many larvae (called 'hydatid sand'). Other animals may then consume the infected organs and the cysts then release proto-scolices. These pass into the small intestine, leading to adult tapeworms.
In humans, the echinococcus eggs invade the small intestine and then enter the circulation. The cysts then locate and reside in organs including the liver, bone, lung and brain. Cysts are usually 1-7 cm but can be as big as 30 cm.
Symptoms
Symptoms depend on the site where the cysts have located and are similar to a growing tumour. Examples include:
Large abdominal cysts which lead to discomfort.
Liver cysts resulting in jaundice.
Lung cysts which can lead to abscess formation.
Brain cysts which can cause focal seizures and raised intracranial pressure.
Cyst content which can lead to anaphylaxis.
Investigations
Eosinophilia.
Abnormal LFTs.
Antibodies against hydatid fluid.
Imaging - eg, CXR, CT scan of the liver or abdomen, brain CT or MRI scan.
Treatment and management
Surgical removal of a cyst or inactivation of a cyst by injection of 10% formalin followed by resection.
Often, complete resection of the cyst is impossible due to close proximity to major vessels.8
Medication may be necessary to keep the cyst from recurring. The drug of choice is albendazole.9
Prevention
Avoid contact with infected animals.
Eliminate the infection in domestic animals.
E. multilocularis
This is similar to E. granulosus with similar morphology and life cycle. It tends to occur in parts of Asia and North America and in Europe too. The intermediate host is rodents. The presentation is similar to E. granulosus but the cysts are multilocular. Again, therapy involves surgery.
E. multilocularis is resistant to praziquantel, although high doses of albendazole or mebendazole may be effective. Prevention involves rodent control measures.
Spirometra spp.
Plerocercoid tapeworm larvae of Spirometra spp. can cause sparganosis, which is rare but has a tendency to affect the following:10
Subcutaneous tissue
Skeletal muscle
Visceral organs
Central nervous system
Spinal cord
Epidemiology
It is found worldwide - most commonly in East Asia. Infection results from:10
Ingesting contaminated water or raw or inadequately cooked flesh of snakes or frogs.
Applying skin of an infected animal to skin as a poultice.
Symptoms
This depends on which area of the body is affected - eg, spinal involvement presents with weakness and paraesthesia.
Investigations
Eosinophilia may not be present if the tapeworm is localised to an organ.
ELISA tests of serum or cerebrospinal fluids to detect antibodies to sparganosis.
Treatment and management
Treatment involves removal of the tapeworm - eg, surgery.
Any surrounding inflammation may require corticosteroids.
Further reading and references
- Tapeworm; World Health Organization.
- Cestodes; Medecins Sans Frontieres.
- Parasites - Taeniasis; Centers for Disease Control and Prevention (CDC).
- Garcia HH, Gonzalez I, Mija L; Neurocysticercosis uncovered by single-dose albendazole. N Engl J Med. 2007 Mar 22;356(12):1277
- British National Formulary (BNF); NICE Evidence Services (UK access only)
- Taeniasis; DPDx, Centers for Disease Control & Prevention
- Rajshekhar V; Purging the worm: management of Taenia solium taeniasis. Lancet. 2004 Mar 20;363(9413):912.
- Diphyllobothriasis; DPDx, Centers for Disease Control & Prevention
- McManus DP, Zhang W, Li J, et al; Echinococcosis. Lancet. 2003 Oct 18;362(9392):1295
- Cerda JR, Buttke DE, Ballweber LR; Echinococcus spp. Tapeworms in North America. Emerg Infect Dis. 2018 Feb;24(2):230-235. doi: 10.3201/eid2402.161126.
- Chautems R, Buhler LH, Gold B, et al; Surgical management and long-term outcome of complicated liver hydatid cysts caused by Echinococcus granulosus. 2005 Mar;137(3):312
- Echinococcosis; DPDx - Centers for Disease Control and Prevention
- Kwon JH, Kim JS; Sparganosis presenting as a conus medullaris lesion: case report and literature review of the spinal sparganosis. Arch Neurol. 2004 Jul;61(7):1126
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 13 Jun 2027
14 Jun 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free