Peak flow recording
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Laurence KnottLast updated 28 Sept 2020
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Peak flow meter for asthma article more useful, or one of our other health articles.
In this article:
Peak flow monitoring is recommended for the ongoing management of asthma and during exacerbations. It is less used these days for the initial diagnosis of asthma, clinicians being encouraged to use more accurate measurements of lung function such as spirometry and the fractional exhaled nitrous oxide (FeNO) test. However, it still has a part to play if diagnostic uncertainty remains after these tests have been completed1 .
There has been much debate in recent years as to whether routine self-monitoring of peak flow for patients with asthma improves management. There is only low-to-moderate evidence that peak flow readings are related to symptoms. Home monitors which provide FEV1 readings are available and give a more accurate assessment of lung function. However, they are expensive. For patients with stable asthma whose symptoms correlate well with peak flow, a peak flow monitor is adequate. Educating the patient in recognition of symptoms which indicate deterioration is nearly as effective.
Peak expiratory flow (PEF) measurement cannot usually be reliably used as the only diagnostic test for chronic obstructive pulmonary disease (COPD) because of its weak specificity. However, one study suggested it could be used to rule out severe to very severe COPD, which may be useful if access to spirometry is limited2 .
Continue reading below
Indications for peak flow recording1 3
PEF measurement is recommended for:
Diagnosis
Peak flow variability should be monitored for 2-4 weeks in adults (aged 17 and over) in whom diagnostic uncertainty remains after initial assessment and a FeNO test, and they have either:
Normal spirometry; or
Obstructive spirometry, reversible airways obstruction but a FeNO level of 39 ppb or less.
A value of more than 20% variability should be regarded as a positive test.
Consider monitoring peak flow variability for 2-4 weeks in adults (aged 17 and over) in whom diagnostic uncertainty remains after initial assessment and a FeNO test and they have either:
Normal spirometry; or
Obstructive spirometry, irreversible airways obstruction and a FeNO level of 35 ppb or more.
A value of more than 20% variability should be regarded as a positive test.
NB: further tests such as estimation of bronchial hyperreactivity using direct bronchial challenge with histamine or methacholine may be required if diagnostic uncertainty remains.
Monitoring
The use of peak flow recording in monitoring asthma must be part of an individual management plan that also includes education and symptom recognition.
Quality-of-life indicators may be as good as peak flow for predicting exacerbations:
Have you had any asthma symptoms during the day?
Have you had any difficulty with sleeping because of symptoms?
Has the asthma interfered with usual activities - eg, work, school?
The patient must have a clear understanding of how to interpret symptoms and peak flow results, and how to use these to adjust treatment and seek medical advice when necessary.
Adults should have their peak flow reassessed every five years, to monitor the decrease in lung function with age.
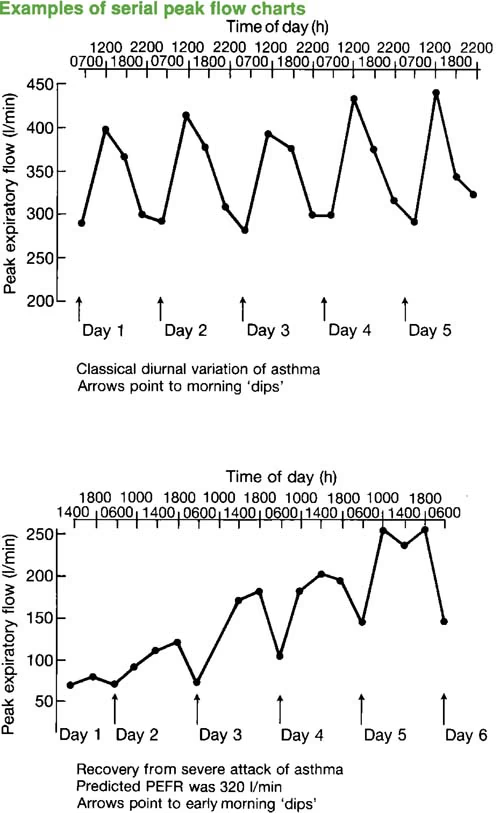
PEAK FLOW CHARTS
Method
Many paediatric and adult patients do not use peak flow meters correctly. It is important to observe how patients use peak flow meters - to detect errors and help ensure correct use and accurate PEF measurements4 .
The patient can be standing or sitting down.
Ensure that the marker on the scale is set to zero.
After a full breath in, the patient should then breathe out with a rapid forced maximal expiratory puff through the mouth and into the meter.
Repeat to give a total of three readings. Take the best reading as the result.
Continue reading below
Self-management plans1
Written personalised action plans as part of self-management education have been shown to improve health outcomes for people with asthma.
They are very important for all patients with asthma, but especially those with moderate-to-severe disease.
Self-management plans improve outcomes such as self-efficacy, knowledge and confidence.
The National Asthma Campaign provides resource materials useful for providing patients with a self-management plan5 . These resource materials can be downloaded.
Peak expiratory flow prediction
You can calculate PEFR here. This calculator inputs race to be able to get a more accurate reading. It can be used in those patients with asthma from ages 5 to 80.
Further reading and references
- DeVrieze BW, Modi P, Giwa AO; Peak Flow Rate Measurement. StatPearls Publishing; 2020 Jan
- Asthma: diagnosis, monitoring and chronic asthma management; NICE Guideline (November 2017 - last updated April 2021)
- Perez-Padilla R, Vollmer WM, Vazquez-Garcia JC, et al; Can a normal peak expiratory flow exclude severe chronic obstructive pulmonary disease? Int J Tuberc Lung Dis. 2009 Mar;13(3):387-93.
- British guideline on the management of asthma; Scottish Intercollegiate Guidelines Network (SIGN), British Thoracic Society (BTS), NHS Scotland (2003 - revised July 2019)
- Self TH, George CM, Wallace JL, et al; Incorrect use of peak flow meters: are you observing your patients? J Asthma. 2014 Aug;51(6):566-72. doi: 10.3109/02770903.2014.914218. Epub 2014 May 9.
- Resources for people with asthma; National Asthma Campaign, Asthma + Lung UK
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 27 Sept 2025
28 Sept 2020 | Latest version

Feeling unwell?
Assess your symptoms online for free