Spinal disc problems
Discitis and back pain red flags
Peer reviewed by Dr Laurence KnottLast updated by Dr Colin Tidy, MRCGPLast updated 15 Feb 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Spinal disc problems article more useful, or one of our other health articles.
In this article:
Disorders affecting intervertebral discs include disc herniation (prolapsed intervertebral disc), degenerative disc disease and infection (discitis).
Spinal disc problems can lead to symptoms of back pain and/or sciatica. There are many other causes of back pain and/or sciatica but they do not primarily originate from the intervertebral discs.
This article focuses on thoracic, lumbar and sacral disc problems. Cervical disc problems are discussed in the separate Cervical Disc Protrusion and Lesions article.
Back pain with/without sciatica is extremely common. Most may be classified as 'simple' back pain where serious underlying pathology is unlikely. However, it is essential always to be aware of 'red flag' warning signs which may merit investigations or even emergency admission.
Continue reading below
Spinal anatomy
The spinal cord is shorter than the spinal canal. The spinal cord ends between the L1 and L2 vertebrae in adults and between L2 and L3 in children. Below the termination of the spinal cord, the nerve roots form the cauda equina which has a horse-tail like appearance. The cauda equina contains the nerve roots L1-L5 and S1-S5. Spinal pathology below L1 of the vertebral column produces mostly lower motor neurone signs.
The intervertebral discs lie between adjacent vertebrae. They consist of a peripheral fibrocartilaginous part called the annulus fibrosus and a central semifluid/gelatinous part - the nucleus pulposus.
Assessment of a patient presenting with back pain and/or sciatica
This is described in detail in the separate Examination of the Spine, Low Back Pain and Sciatica and Neurological Examination of the Lower Limbs articles.
Back pain red flags1
Red flags that suggest cauda equina syndrome include:
Severe or progressive bilateral neurological deficit of the legs, such as major motor weakness with knee extension, ankle eversion, or foot dorsiflexion.
Recent-onset urinary retention (caused by bladder distension because the sensation of fullness is lost) and/or urinary incontinence (caused by loss of sensation when passing urine).
Recent-onset faecal incontinence (due to loss of sensation of rectal fullness).
Perianal or perineal sensory loss (saddle anaesthesia or paraesthesia).
Unexpected laxity of the anal sphincter.
Red flags that suggest spinal fracture include:
Sudden onset of severe central spinal pain which is relieved by lying down.
History of major or minor trauma, or even just strenuous lifting in people with osteoporosis.
Structural deformity of the spine (eg, a step from one vertebra to an adjacent vertebra).
Point tenderness over the vertebral body, or pathological fracture.
Red flags that suggest cancer or infection (such as discitis, vertebral osteomyelitis, or spinal epidural abscess) include:
Onset in people older than 50 years, or younger than 20 years of age.
Pain that remains when supine, aching night pain that disturbs sleep, and thoracic pain.
Past history of cancer (breast, lung, gastrointestinal, prostate, renal, and thyroid cancers are more likely to metastasise to the spine).
Fever, chills or unexplained weight loss.
Recent infection (eg, urinary tract infection).
Intravenous drug misuse.
Immunocompromise such as HIV infection.
Red flags that suggest spondyloarthropathy include:
Early morning stiffness lasting >45 minutes.
Night pain.
'Gelling'.
Easier with movement/worse after rest.
Red flags that suggest a high risk of permanent damage to the compressed nerve include:
Significant muscle weakness or wasting.
Loss of tendon reflexes.
Presence of a positive Babinski reflex (toes extend and fan outwards when the lateral part of the sole of the foot is stimulated).
Continue reading below
When to refer someone with low back pain/sciatica1
If red flag symptoms and signs that may suggest a serious underlying cause (see above), admit or refer urgently for specialist assessment using clinical judgement.
Arrange emergency referral to a spinal surgery service if there is suspicion of:
Cauda equina syndrome.
Acute spinal cord compression: new/progressive widespread neurological deficit.
Progressive limb weakness including major motor radiculopathy.
Arrange urgent referral to a spinal surgery service or urgent MRI (within two weeks) if:
There is suspicion of tumour or infection.
Red flags are present in the absence of neurological dysfunction.
Seek advice from the emergency spinal surgery service for people with severe or progressive motor deficit (for example, foot drop).
Consider offering referral:
For a group exercise programme.
To a physiotherapist, but only as part of a treatment package including exercise with or without psychological therapy.
For psychological therapies using a cognitive behavioural approach, but only as part of a treatment package including exercise, with or without manual therapy.
Prolapsed intervertebral disc1
See also the separate articles on Cervical Disc Protrusion and Lesions and Low Back Pain and Sciatica.
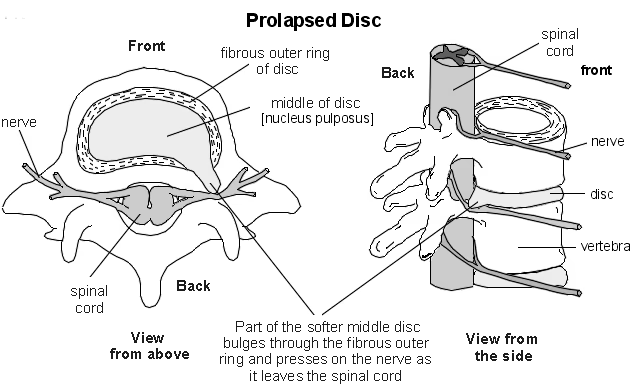
The nucleus pulposus of the spinal disc is usually contained by the annulus fibrosus. If the nucleus herniates, it can irritate and/or compress the adjacent nerve root, causing symptoms of sciatica.
Traumatic disc herniation can occur. Spinal disc herniation can also occur secondary to degenerative disc disease.
A herniated nucleus pulposus is most common in those aged below 40 years, whilst degeneration of discs tends to affect those aged over 40 years, with the prevalence increasing with advancing age. Spinal disc lesions of the lumbar spine are more common than those of the cervical spine and disc lesions of the thoracic spine are rare.
The term sciatica is used for the pain, tingling and numbness that arise due to nerve root entrapment in the lumbosacral spine. The symptoms may be felt in one or more of the lumbar nerve roots. About 90% of cases of sciatica are caused by a herniated intervertebral disc. This most commonly occurs at the L5/S1 level. See also the separate Low Back Pain and Sciatica article.
Above and side views
Presentation
Lumbosacral disc herniation
If there is nerve entrapment in the lumbosacral spine, this leads to symptoms of sciatica which include:1
Unilateral leg pain which radiates below the knee to the foot/toes.
The leg pain being more severe than the back pain.
Numbness, paraesthesia, weakness and/or loss of tendon reflexes, which may be present and are found in the same distribution and only in one nerve root distribution.
A positive straight leg raising test (there is greater leg pain and/or more nerve compression symptoms on raising the leg).
Pain which is usually relieved by lying down and exacerbated by long walks and prolonged sitting.
The functional distribution of the lumbar nerve roots and the sciatic nerve are detailed in the separate Low Back Pain and Sciatica article.
Large herniations can compress the cauda equina, leading to symptoms/signs of saddle anaesthesia, urinary retention and incontinence as described above.
Symptoms tend at least to resolve partially in 66% of people with a disc herniation, after six months. This is because the herniated portion tends to regress over time.2
However, nerve root compression can lead to permanent nerve damage with sensory and motor deficit.1
Thoracic disc herniation
Spinal disc problems in the thoracic spine can lead either to nerve root irritation or to cord compression.
Thoracic spine lesions can present with symptoms similar to lumbar disc lesions.
In nerve root irritation, there may be shooting pain down the legs.
There may be pain, paraesthesia or dysaesthesia in a dermatomal distribution.
A thoraco-abdominal sensory examination can help to determine the level of the lesion: the nipple is innervated by T4; the xiphoid by T7; the umbilicus by T10; the inguinal region by T12.
Testing of the abdominal and cremasteric reflexes can help to identify myelopathy and cord compression.
Cord compression:
This is a neurosurgical emergency.
Cord compression in the thoracic spine can produce paraplegia.
There may be clonus or a positive Babinski reflex.
There may be bladder/bowel dysfunction.
Herniation of T2-T5 can mimic cervical disc disease.
Investigation
No investigation may be needed if symptoms settle within six weeks.
MRI is very sensitive in showing disc herniations.
CT myelography may also be used.
Plain X-rays are sometimes useful, as they can show misalignments, instabilities and congenital anomalies well.
Management1
Spinal cord compression or cauda equina syndrome are neurological emergencies that require immediate referral and intervention.
Analgesia:
Simple analgesics as first line (paracetamol/non-steroidal anti-inflammatory drug). These may be used in combination.
A weak opioid such as codeine or tramadol may be added if pain is still present.
Consider a benzodiazepine (eg, diazepam) if there is muscle spasm.
Consider a trial of a tricyclic antidepressant or gabapentin if there is persistent sciatica.
If stronger analgesia is needed, refer to a pain clinic/specialist service.
Encouragement to keep active: swimming is a good exercise.
Heat and massage may relieve muscle spasm.
Avoidance of activities that may aggravate pain - eg, lifting, prolonged sitting.
Physiotherapy.
Surgery:3
Pain due to a herniated lumbosacral disc may settle within six weeks. If it does not, or there are back pain red flags such as the possibility of cauda equina syndrome, referral to an orthopaedic surgeon or a neurosurgeon should be considered.
Interventions for people with chronic intractable pain or neurological complications include removal of the protruding disc (discectomy) and/or spinal fusion.
The National Institute for Health and Care Excellence (NICE) recommends that prosthetic intervertebral disc replacement may be used in the treatment of symptomatic degenerative disc disease of the lumbar spine.
NICE recommends that percutaneous intradiscal laser ablation in the lumbar spine may be considered as a treatment option.4
The current evidence of percutaneous endoscopic laser lumbar discectomy is inadequate for it to be considered as a treatment option.5
Complications1
Permanent nerve damage with sensory deficits and/or permanent motor weakness.
Psychosocial problems.
Loss of employment.
Prognosis1
The prognosis for acute sciatica is favourable for most people. The herniated portion of an intervertebral disc causing sciatica tends to regress over time and 66% of people have at least partial resolution after six months.
About 50% of people with acute sciatica report some improvement within ten days and about 75% report some improvement after four weeks. However, up to 30% of people continue to have pain for one year or longer.
The prognosis is worse for women and people who initially have greater disability or pain
Prevention
Regular exercise.
Weight loss if overweight.
Safe lifting techniques.
Correct sitting position and posture.
Continue reading below
Degenerative disc disease6
Intervertebral disc degeneration is one of the major causes of low back pain.
The exact cause of this is not known. Some suggest that degenerative disc disease is a natural part of ageing; however, disc degeneration can also occur in young people. The cause of degenerative disc disease is likely to be multifactorial, including genetic, environmental, traumatic, inflammatory, infectious and other factors.
Annular tears, internal disc disruption and resorption, disc space narrowing, disc fibrosis and osteophyte formation can all occur.
Degenerative disc disease may lead to disc herniation.
Discitis7 8 9
Spondylodiscitis describes infection of both the intervertebral disc space and the adjacent vertebrae.
Pyogenic infections of the spine are relatively rare with an incidence between 1 in 100,000 and 1 in 250,000 per year but the incidence is increasing due to increases in average life-expectancy and medical comorbidities.
Discitis pathophysiology
Discitis is inflammation of the vertebral disc space. It is usually associated with infection and can co-exist with vertebral osteomyelitis (spondylodiscitis).
Discitis most commonly affects the lumbar spine. The thoracic spine is least commonly affected with the cervical spine between the two.
There is usually haematogenous spread of infection from other parts of the body. The urinary tract, lungs and soft tissues are common primary sites for infection. It may be difficult to find a primary site.
Staphylococcus aureus is the most common pathogen.
Discitis can occur in children but most commonly affects males aged in their 50s.
Risk factors include any cause of immunosuppression (including diabetes) and intravenous drug use.
Discitis may rarely follow surgery involving the disc space.
Discitis presentation
Discitis diagnosis is difficult and often delayed or missed due to the rarity of the disease and the high frequency of low back pain in the general population.
An insidious onset is common, with neck or back pain and localised tenderness. Pain is worse on movement. Mobility may be restricted.
There may be associated fever and weight loss.
Neurological deficit may be present. This is more likely in the cervical spine.
Investigations
ESR and CRP are raised. They can be used to monitor response to treatment.
White blood cell count may be normal.
Blood cultures, sputum, urine and any other appropriate cultures should be taken to look for the source of infection.
X-ray of the spine may show disc space narrowing, end-plate irregularities and annulus calcification. Osteomyelitis changes may be seen including decreased bone density and bone destruction. However, X-ray may be normal initially.
Nuclear medicine scans may be helpful.
CT and MRI scanning show changes earlier than plain X-ray. MRI is the most sensitive and specific.
CT-guided or open biopsy of the infected disc space area can provide histological confirmation of discitis and allow culture. Surgical debridement may be carried out at the same time.
Discitis management
Antibiotics are needed. These should be adjusted if/when culture results are available. Parenteral treatment is usually used and may be needed for 6-8 weeks. ESR can be used to monitor response.
Immobilisation: two weeks of bed rest have been suggested, followed by immobilisation with a brace, which may be needed for 3-6 months.
Analgesia should be prescribed as required.
Surgical treatment may be needed if there is neurological deficit, spinal deformity or lack of response to antibiotic treatment.
Discitis prognosis
Antibiotic treatment with/without surgery is usually successful in treating the condition. However, a minority will have permanent neurological deficits.
Complications can include spread of infection into the epidural space or paraspinal soft tissues.
Mortality is reported as about 2%.
Further reading and references
- Low back pain and sciatica in over 16s: assessment and management; NICE Guidelines (November 2016 - last updated December 2020)
- Sciatica (lumbar radiculopathy); NICE CKS, October 2021 (UK access only)
- Jordan J, Konstantinou K, O'Dowd J; Herniated lumbar disc. BMJ Clin Evid. 2011 Jun 28;2011. pii: 1118.
- Prosthetic intervertebral disc replacement; NICE Interventional Procedure Guidance, July 2009
- Percutaneous intradiscal laser ablation in the lumbar spine; NICE Interventional Procedure Guidance, September 2010
- Epiduroscopic lumbar discectomy through the sacral hiatus for sciatica; NICE Interventional procedures guidance, December 2016
- Molinos M, Almeida CR, Caldeira J, et al; Inflammation in intervertebral disc degeneration and regeneration. J R Soc Interface. 2015 Mar 6;12(104):20141191. doi: 10.1098/rsif.2014.1191.
- Zarghooni K, Rollinghoff M, Sobottke R, et al; Treatment of spondylodiscitis. Int Orthop. 2012 Feb;36(2):405-11. doi: 10.1007/s00264-011-1425-1. Epub 2011 Dec 6.
- Gouliouris T, Aliyu SH, Brown NM; Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010 Nov;65 Suppl 3:iii11-24.
- Kapsalaki E, Gatselis N, Stefos A, et al; Spontaneous spondylodiscitis: presentation, risk factors, diagnosis, management, and outcome. Int J Infect Dis. 2009 Sep;13(5):564-9. doi: 10.1016/j.ijid.2008.08.025. Epub 2008 Dec 13.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 14 Feb 2027
15 Feb 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free