Acromioclavicular joint problems
Peer reviewed by Dr Sarah Jarvis MBE, FRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 27 Apr 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Shoulder pain article more useful, or one of our other health articles.
In this article:
Pnonyms: collar bone/clavicle disorders
Continue reading below
What is the acromioclavicular joint?
The acromioclavicular (AC) joint is the articulation between the acromion process of the scapula and the lateral end of the clavicle. It is one of the important functional joints that allows a full range of movement at the glenohumeral joint. A joint capsule and several ligaments hold the joint in situ, assisted by the trapezoid and conoid coracoclavicular (CC) ligaments that connect the coracoid process of the scapula to the mid/lateral clavicle. The joint contains a fibrocartilaginous disc that cushions the articulations.
Epidemiology1
Most injuries affecting the acromioclavicular joint occur in males with a male to female ratio of approximately 5:1. The most common age group affected is those in their 20s.2
In the general population the incidence of acromioclavicular joint dislocation is 3-4 per 100,000, with 25% to 52% occurring during sporting activities.
acromioclavicular joint injuries are especially prevalent among players of high-impact contact sports3 but also occur after road traffic accidents and falling from a bike.
One series found that 41% of collegiate American football players had suffered an AC separation.4
Continue reading below
Acromioclavicular joint pain causes5
See also the separate Shoulder Pain article.
There are two broad causes of acromioclavicular joint problems:
AC joint disruption - when trauma leads to varying degrees of displacement of the distal clavicle from the local ligaments and muscles.
Osteoarthritis (OA) and/or osteolysis of the AC joint.
Acromioclavicular joint disruption
Mechanism of injury
Acromioclavicular joint injuries represent nearly half of all athletic shoulder injuries, often resulting from a fall on to the tip of the shoulder with the arm in adduction, or a direct blow to the acromion with the humerus adducted, as in collision in high-impact contact sports.3
Injury may occur as a consequence of throwing sports or chronic irritation due to activities that require repetitive overhead motions, particularly weightlifting. Its aetiology is uncertain but may be due to repeated stress fractures of the lateral clavicle.
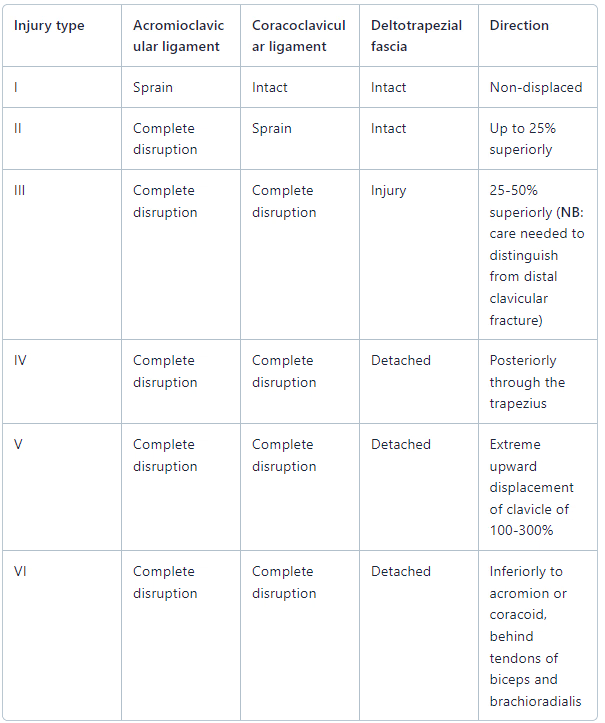
Injury classification1 6
Acromioclavicular joint disruption (Rockwood Classification)
Continue reading below
Osteoarthritis and distal clavicular osteolysis
OA of the acromioclavicular joint may occur after injury, repetitive overuse or, more rarely, as a primary phenomenon. It commonly occurs in middle age, due to degeneration of the fibrocartilaginous disc.7
Distal clavicular osteolysis may occur:8
Spontaneously in rheumatoid arthritis, hyperparathyroidism, gout, multiple myeloma, systemic sclerosis and massive essential osteolysis (Gorham's disease).
Due to infection.
Particularly in upper limb weight training and also in those who are involved in throwing sports.
Acromioclavicular joint pain symptoms and signs
See also the separate Shoulder Examination article.
Acromioclavicular joint disruption
There will usually be a history of relevant trauma and severe pain over the lateral shoulder.
There may be marked tenderness of the acromioclavicular joint and a visible/palpable 'step' if there is clavicular separation. This is best viewed with the arm adducted across the body.
The position of the clavicle should be determined along its whole length (associated sternoclavicular abnormalities may occur as well as fracture of clavicle).
Brachial and radial pulses should be checked along with sensory and motor function in the affected arm, due to the possibility of injury to brachial plexus and axillary/subclavian vessels.
Patients may also present with acute complications of acromioclavicular joint disruption - for example:
Injury to axillary/subclavian vessels.
Injury to brachial plexus.
Muscular avulsion, particularly deltoid and trapezius.
Rarely, pneumothorax if there is associated clavicular fracture.
OA and distal clavicular osteolysis
Diffuse lateral shoulder pain and/or localised acromioclavicular joint pain.
May be simply an ache in the deltoid area.
Often worse at night.
Local tenderness with exacerbation on passive and active shoulder movements.
Cross-adduction (ie reach over front of opposite shoulder) often worsens pain; further passive cross-adduction by the examiner may aggravate this.
It is important to differentiate OA from instability.
Reduced range of movement is rare unless there is a prolonged period of arthritis.
Differential diagnosis9 10
Clavicular fracture.
Rotator cuff disorders (especially in cases of OA and osteolysis).
Other causes of shoulder pain
Diagnostic imaging1 10 11
Plain radiographs are the initial choice.
Type I and II injuries may be differentiated using stressed radiographs where weights are hung from the patient's wrists, although many consider this technique to be unhelpful.
A Zanca view (AP view where the X-ray beam is directed at the AC joint with 10° cephalic tilt) optimises the view of the joint.
CXR or full clavicle views may be needed in some cases.
Carefully inspect the scapula to rule out associated scapular fracture.
A variety of images may be required to assess the degree of AC joint disruption; an axial view of the shoulder is important in differentiating between a type III and a type IV injury.
OA of the AC joint cannot be reliably diagnosed by X-ray as, although degeneration may be revealed, similar findings can be seen in asymptomatic individuals.7
Acromioclavicular joint pain treatment and management1 12 13
Acromioclavicular joint disruption
Types I and II injuries:
Generally respond favourably to conservative management:
Ice, a sling for 1-3 weeks and analgesia/non-steroidal anti-inflammatory drug (NSAID) followed by physiotherapy to strengthen muscles and ligaments after the acute phase.
If symptoms are not resolving, it is important to ensure that a superior labral tear anterior to posterior (SLAP) or rotator cuff injury has not also occurred.
The most common cause of persisting discomfort is scapular dyskinesia which will require a scapular stabilisation programme
Type III injuries:14
Management is controversial.
Conservative treatment shows excellent results with painless shoulder function but there may be significant deformity. However, some patients experience chronic instability and pain; it is currently not possible to identify those patients who will decompensate their shoulder biomechanics.
There are wide geographical differences, with the majority of type III injuries in Germany being treated surgically, whereas in the USA, conservative management is favoured
No randomised controlled trials have been published regarding the management of type III injuries.
Types IV to VI:
Treated surgically except in selected elderly patients, when functional restoration may be possible with conservative treatment due to their reduced physical activities.
Various surgical techniques are used, both open and laparoscopic.
There is a lack of high-quality evidence regarding which operation(s) have the best outcomes. Surgical options include:
Rigid AC fixation with a Hook plate or screw.
Weaver-Dunn procedure, using the coraco-acromial ligament to substitute the torn CC ligament.
Non-rigid CC fixation with tendon graft or synthetic materials (rigid fixation with screws is associated with a high risk of breakage or loosening).
CC ligament reconstruction.
All acute lesions thought to be worse than type II should be referred urgently for an orthopaedic opinion.
OA/osteolysis
Activity modification, physiotherapy and NSAID/other analgesia.
Intra-articular corticosteroids may provide relief of symptoms for up to three months in expert hands. Currently there is no consensus in terms of dosage, and injections should be limited to fewer than four per year.15 Duration of analgesia is very variable with ranges of two hours to three months reported.
In severe cases of OA or osteolysis, distal clavicular resection may need to be considered. This can be performed openly or arthroscopically.7
Late complications
Impingement syndrome of the supraspinatus tendon, due to narrowing of the scapular outlet.
OA of the acromioclavicular joint.
Frozen shoulder and chronic shoulder pain/limitation of movement.
Further reading and references
- Woodmass JM, Esposito JG, Ono Y, et al; Complications following arthroscopic fixation of acromioclavicular separations: a systematic review of the literature. Open Access J Sports Med. 2015 Apr 10;6:97-107. doi: 10.2147/OAJSM.S73211. eCollection 2015.
- LeVasseur MR, Mancini MR, Berthold DP, et al; Acromioclavicular Joint Injuries: Effective Rehabilitation. Open Access J Sports Med. 2021 May 28;12:73-85. doi: 10.2147/OAJSM.S244283. eCollection 2021.
- Kiel J, Kaiser K; Acromioclavicular Joint Injury. StatPearls, Aug 2021.
- Babhulkar A, Pawaskar A; Acromioclavicular joint dislocations. Curr Rev Musculoskelet Med. 2014 Mar;7(1):33-9. doi: 10.1007/s12178-013-9199-2.
- White B, Epstein D, Sanders S, et al; Acute acromioclavicular injuries in adults. Orthopedics. 2008 Dec;31(12). pii: orthosupersite.com/view.asp?rID=34696.
- Simovitch R, Sanders B, Ozbaydar M, et al; Acromioclavicular joint injuries: diagnosis and management. J Am Acad Orthop Surg. 2009 Apr;17(4):207-19.
- Kaplan LD, Flanigan DC, Norwig J, et al; Prevalence and variance of shoulder injuries in elite collegiate football players. Am J Sports Med. 2005 Aug;33(8):1142-6. Epub 2005 Jul 7.
- Buttaci CJ, Stitik TP, Yonclas PP, et al; Osteoarthritis of the acromioclavicular joint: a review of anatomy, biomechanics, diagnosis, and treatment. Am J Phys Med Rehabil. 2004 Oct;83(10):791-7.
- Saccomanno MF, DE Ieso C, Milano G; Acromioclavicular joint instability: anatomy, biomechanics and evaluation. Joints. 2014 Jul 8;2(2):87-92. doi: 10.11138/jts/2014.2.2.087. eCollection 2014 Apr-Jun.
- Mall NA, Foley E, Chalmers PN, et al; Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med. 2013 Nov;41(11):2684-92. doi: 10.1177/0363546513485359. Epub 2013 May 6.
- Schwarzkopf R, Ishak C, Elman M, et al; Distal clavicular osteolysis: a review of the literature. Bull NYU Hosp Jt Dis. 2008;66(2):94-101.
- Monica J, Vredenburgh Z, Korsh J, et al; Acute Shoulder Injuries in Adults. Am Fam Physician. 2016 Jul 15;94(2):119-27.
- Shoulder pain; NICE CKS, April 2017 (UK access only)
- Krill MK, Rosas S, Kwon K, et al; A concise evidence-based physical examination for diagnosis of acromioclavicular joint pathology: a systematic review. Phys Sportsmed. 2018 Feb;46(1):98-104. doi: 10.1080/00913847.2018.1413920. Epub 2017 Dec 13.
- Modi CS, Beazley J, Zywiel MG, et al; Controversies relating to the management of acromioclavicular joint dislocations. Bone Joint J. 2013 Dec;95-B(12):1595-602. doi: 10.1302/0301-620X.95B12.31802.
- Jeong JY, Chun YM; Treatment of acute high-grade acromioclavicular joint dislocation. Clin Shoulder Elb. 2020 Sep 1;23(3):159-165. doi: 10.5397/cise.2020.00150. eCollection 2020 Sep.
- Korsten K, Gunning AC, Leenen LP; Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. Int Orthop. 2014 Apr;38(4):831-8. doi: 10.1007/s00264-013-2143-7. Epub 2013 Oct 31.
- Skedros JG, Hunt KJ, Pitts TC; Variations in corticosteroid/anesthetic injections for painful shoulder conditions: comparisons among orthopaedic surgeons, rheumatologists, and physical medicine and primary-care physicians. BMC Musculoskelet Disord. 2007 Jul 6;8:63.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 28 Mar 2027
27 Apr 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free