Torsades de pointes
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 30 Nov 2022
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Abnormal heart rhythms article more useful, or one of our other health articles.
In this article:
Continue reading below
What is torsades de pointes?
Torsades de pointes is a distinctive polymorphic ventricular tachycardia in which the QRS amplitude varies and the QRS complexes appear to twist around the baseline. Torsades de pointes is associated with a prolonged QT interval, which may be congenital or acquired.1 2
Is torsades de pointes fatal?
Torsades de pointes is usually not sustained and terminates spontaneously but frequently recurs unless the underlying cause is corrected. Torsades de pointes may degenerate into sustained ventricular tachycardia or ventricular fibrillation. Torsades is a life-threatening arrhythmia and may present as sudden cardiac death in patients with structurally normal hearts.3
Torsades de pointes
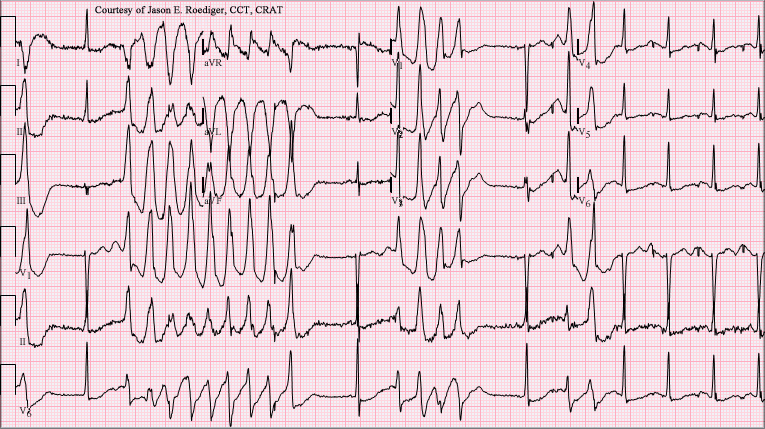
By Jer5150, CC BY-SA 3.0, via Wikimedia Commons
Continue reading below
How common is torsades de pointes?4
Genetic polymorphisms that lead to QT prolongation (and so predispose to torsades de pointes) have been identified.5 However there is currently inconsistent evidence to identify a single population as being more at risk than an other.
Torsades occurs at any age. If it occurs at an early age, the cause is usually due to congenital long QT syndrome. In later years, the cause is usually due to acquired long QT syndrome.
Risk factors
Congenital long QT syndromes - eg, Jervell and Lange-Nielsen syndrome, Romano-Ward syndrome.6 7
Acquired long QT syndromes:
Drugs - eg, antiarrhythmic agents of classes Ia and III, erythromycin, ketoconazole, tricyclic antidepressants, methadone, antipsychotics.8
Electrolyte disturbances; hypokalaemia, hypomagnesaemia, hypocalcaemia.
Metabolic; hypothyroidism, anorexia nervosa, malnutrition.
Bradycardia; sinoatrial disease, atrioventricular (AV) block.
Toxins; heavy metals, insecticides.
Torsades de pointes symptoms9
About 50% of people with torsades de pointes are asymptomatic.
Episodes of torsades in patients with congenital long QT syndromes may be triggered by stress, fear or physical exertion.
Patients with torsades usually present with recurrent episodes of palpitations, dizziness, and syncope. Sudden cardiac death can occur with the first episode and is the presenting feature in up to 10% of cases.
Nausea, pallor, cold sweats, shortness of breath and chest pain may occur.
A history of congenital deafness or a family history of sudden death may indicate a congenital long QT syndrome.
Physical findings depend on the rate and duration of tachycardia and the degree of cerebral hypoperfusion. Findings include rapid pulse, low or normal blood pressure, and transient or prolonged loss of consciousness.
Other physical signs depend on the cause - eg, features of a congenital disorder.
Continue reading below
Differential diagnosis9
Supraventricular tachycardia with aberrant conduction.
Other causes of syncope or sudden cardiac death.
Drug toxicity.
Investigations
Paroxysms of 5-20 beats, with a heart rate faster than 200 beats per minute. Sustained episodes are occasionally seen.
Progressive change in polarity of QRS about the isoelectric line occurs with complete 180° twist of QRS complexes in 10-12 beats.
Usually, a prolonged QT interval and pathological U waves are present.3 The most consistent indicator of QT prolongation is a QT of 0.60 seconds or longer or a QTc (corrected for heart rate) of 0.45 seconds or longer. QTc = QT interval divided by the square root of the interval (in seconds) between the onset of each QRS complex (Bazett's formula).
A short-long-short sequence between the R-R interval occurs before the trigger response.
Electrolytes; hypokalaemia, hypomagnesaemia and hypocalcaemia.
Cardiac enzymes; assessment for myocardial ischaemia.
CXR and echocardiography, to rule out structural heart disease.
How to treat torsades de pointes11
Short-term treatment
Defibrillation:
Although torsades is often self-terminating, it may develop into ventricular fibrillation, which requires defibrillation.12
In an otherwise stable patient, direct current (DC) cardioversion is usually a last resort because torsades is paroxysmal in nature and frequently recurs after cardioversion.
Discontinuation of any offending agent (stop all QT-prolonging drugs) and correction of any underlying cause such as hypokalaemia, hypomagnesaemia and bradycardia.
Intravenous magnesium is the drug of choice for torsades de pointes. Magnesium is effective even in patients with normal magnesium levels.
Acceleration of the heart rate can be achieved by using beta 1-adrenergic agonists such as isoprenaline or overdrive electrical pacing.
Isoprenaline is used as an interim treatment until overdrive pacing can be started:
Isoprenaline accelerates AV conduction and decreases the QT interval.
It can be used in bradycardia-dependent torsades that is usually associated with acquired long QT syndrome.
Isoprenaline is given as a continuous intravenous infusion to keep the heart rate faster than 90 beats per minute.
Beta-adrenergic agonists are contra-indicated in the congenital form of long QT syndrome.
Pacing can be effective in terminating torsades by increasing the heart rate and so reducing the QT interval.
Atrial pacing is the preferred mode because it preserves the atrial contribution to ventricular filling. In patients with AV block, ventricular pacing can be used to suppress torsades.
Long-term treatment
Patients without syncope, ventricular tachyarrhythmia or a family history of sudden cardiac death can be observed without starting any treatment.
Congenital long QT syndrome:
Beta-adrenergic antagonists are used as a first-line long-term therapy in congenital long QT syndrome. Propranolol is has been the most extensively used.
Beta-blockers are contra-indicated in acquired cases because bradycardia produced by these agents can precipitate torsades. They should also be avoided in those congenital cases in which bradycardia is a prominent feature.
Permanent pacing benefits patients who remain symptomatic despite receiving the maximally tolerated dose of beta-blockers and can be used in addition to beta-blockers.
High left thoracic sympathectomy is effective in patients who remain refractory to beta-blockade and pacing.
Implantable cardioverter-defibrillators (ICDs) are useful in rare instances when torsades still continues despite all of these treatments. Beta-blockers should be used along with ICDs because shock can further precipitate torsades by adrenergic stimulation.
Acquired long QT syndrome:
Long-term treatment in acquired cases is usually not required because the QT interval returns to normal once the predisposing factor has been corrected.
Pacemaker implantation is effective in cases that are associated with heart block or bradycardia.
ICDs are indicated in cases that cannot be managed by avoidance of any specific precipitating factor.
Complications9
Prognosis
Patients may revert spontaneously or convert to a non-polymorphic ventricular tachycardia or ventricular fibrillation.12
Torsades is a life-threatening arrhythmia and may present as sudden cardiac death in patients with structurally normal hearts.
In acquired long QT syndrome, the prognosis is excellent once any precipitating factor has been removed.
Prevention12
Avoid offending drugs that prolong the QT interval.
Prevent predisposing conditions such as hypokalaemia, hypomagnesaemia, and hypocalcaemia, especially in patients shown to have long QT interval.
Screen families of patients with torsades for whom the cause for prolonged QT is suggested to be congenital.
Further reading and references
- Scheinman M, Bunch TJ, Singh M; A tale of 2 torsades: How to approach a patient with torsades de pointes and distinguish between classical and pseudo-torsades de pointes. HeartRhythm Case Rep. 2022 Apr 15;8(4):305-308. doi: 10.1016/j.hrcr.2022.03.007. eCollection 2022 Apr.
- Kaye AD, Volpi-Abadie J, Bensler JM, et al; QT interval abnormalities: risk factors and perioperative management in long QT syndromes and Torsades de Pointes. J Anesth. 2013 Aug;27(4):575-87. doi: 10.1007/s00540-013-1564-1. Epub 2013 Feb 15.
- Trinkley KE, Page RL 2nd, Lien H, et al; QT interval prolongation and the risk of torsades de pointes: essentials for clinicians. Curr Med Res Opin. 2013 Dec;29(12):1719-26. doi: 10.1185/03007995.2013.840568. Epub 2013 Sep 23.
- Baldzizhar A, Manuylova E, Marchenko R, et al; Ventricular Tachycardias: Characteristics and Management. Crit Care Nurs Clin North Am. 2016 Sep;28(3):317-29. doi: 10.1016/j.cnc.2016.04.004. Epub 2016 Jun 22.
- Sauer AJ, Newton-Cheh C; Clinical and genetic determinants of torsade de pointes risk. Circulation. 2012 Apr 3;125(13):1684-94. doi: 10.1161/CIRCULATIONAHA.111.080887.
- Kallergis EM, Goudis CA, Simantirakis EN, et al; Mechanisms, risk factors, and management of acquired long QT syndrome: a comprehensive review. ScientificWorldJournal. 2012;2012:212178. doi: 10.1100/2012/212178. Epub 2012 Apr 19.
- Pabba K, Chakraborty RK; Jervell and Lange Nielsen Syndrome
- Homma K; The Pathological Mechanisms of Hearing Loss Caused by KCNQ1 and KCNQ4 Variants. Biomedicines. 2022 Sep 12;10(9). pii: biomedicines10092254. doi: 10.3390/biomedicines10092254.
- Heemskerk CPM, Pereboom M, van Stralen K, et al; Risk factors for QTc interval prolongation. Eur J Clin Pharmacol. 2018 Feb;74(2):183-191. doi: 10.1007/s00228-017-2381-5. Epub 2017 Nov 22.
- Cohagan B, Brandis D; Torsade de Pointes
- ECG Library
- Al-Khatib SM, Stevenson WG, Ackerman MJ, et al; 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2018 Oct;15(10):e190-e252. doi: 10.1016/j.hrthm.2017.10.035. Epub 2017 Oct 30.
- Drew BJ, Ackerman MJ, Funk M, et al; Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. J Am Coll Cardiol. 2010 Mar 2;55(9):934-47. doi: 10.1016/j.jacc.2010.01.001.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 29 Nov 2027
30 Nov 2022 | Latest version

Feeling unwell?
Assess your symptoms online for free