Contrast Sensitivity – Vivity vs. Eyhance vs. Tecnis (ZCBOO) vs. Arysof (SN60WF)
Posted , 13 users are following.
I was interested in Vivity but the warning about Contrast Sensitivity concerned me. So I started looking into Eyhance. It's very difficult to compare IOL metrics since the data comes from all difference sources and often uses different testing configurations. And some data can only be sourced if you're a researcher or pay money for a paper. But I think I have it figured out. Here are some of my sources:
.
Eyhance Specs from J&J
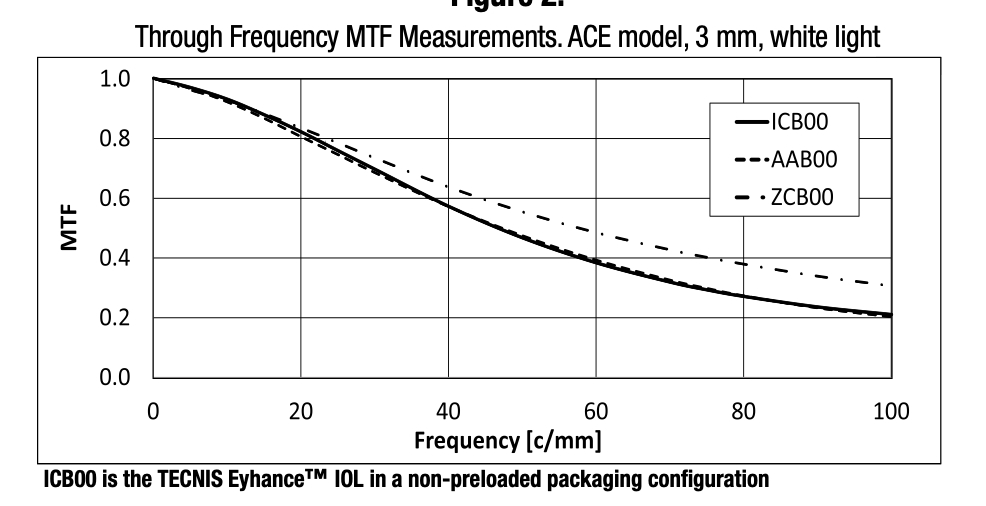
Go to jnjvisionpro and look in Products > Eyhance for a spec sheet with a defocus curve and graph of Through Frequency MTF Measurements. ACE model, 3 mm, white light graph (below)
FDA approval PDF for Vivity (Page 8)
Search on "P930014S126B" but only at 50 lp/mm and only for a 3mm (daylight conditions) pupil.
Eyhance Whitepaper from The Optomologist dotcom
Search on "Delivering intermediate vision the new tecnics eyhance monofocal iol"
There seem to be two ways to test Contrast Sensitivity, a lab test using an "ACE" model eye and actual people in a room looking at a chart trying to make out patterns of vertical lines. The former lp/mm units(?). The latter uses lines per degree. I managed to find data for all 4 lenses mentioned in the subject of this thread for the first kind of test (lp/mm). This is what I found. Sometimes I'm guessing at these numbers based on a visual graph.
.
MTF 50 lp/mm at distance
.
3mm (day)
Tecnis: 0.56
Acrysof: 0.46
Eyhance: 0.46
Vivity: 0.25
.
5mm (night)
Tecnis: 0.42
Eyhance: 0.36
Acrysof: 0.28
Vivity: ???
.
Vivity did OK in second kind of test (people in a room reading a chart) in binocular mesopic conditions. You can find that data in the FDA PDF as well as a presentation that you can find by searching on "Cathleen Mccabe ISO presentation". The presentation says the CS loss in binocular mesopic conditions is not "clinically significant" but it still concerns me.
.
For discussion... should these lab-based measurements (using an ACE model eye) be taken with a grain of salt? Am I making myself crazy over nothing? Is it better to just focus on real world results and patient testimonials?
.
If any of my numbers are wrong or if anyone finds more or better data please reply.
1 like, 41 replies
xen42188 Guest
Edited
david, ACE model and the ISO model used by thr FDA have slight differences. ACE slightly favours Tecnis in that it factors in spherical aberration. AcrySof mono (SN) and Tecnis mono are comparable so I'd just look at your second chart to draw conclusions about MTF loss in Vivity.
RonAKA Guest
Edited
That is good information for thought. I always like to use the "does that make basic sense" question when trying to make sense of technical issues like this. For me the one nagging question is why would the Tecnis Eyhance be better than the monofocal IQ Aspheric lens (SN60WF)? That does not seem to make sense unless the overall light transmission of the non blue light filtered Eyhance lens gives it a big advantage in the test procedure used. The Eyhance is modifying asphericity to give more depth of focus but the SN60WF is not.
.
Since I already have the SN60WF lens in one eye and am considering either the same lens or the Vivity in the second eye, I am not sure what to make of the loss of contrast sensitivity with the Vivity. Alcon claims the loss is reduced and not clinically significant if you have the Vivity in both eyes. I presume that is because binocular vision is always better than monocular. What I am thinking is that contrast sensitivity will probably be better with the SN60WT combined with the Vivity, than it would be with both Vivity lenses? Your thoughts?
Guest
Edited
I just watched a webinar on YouTube about Eyhance (presentation of the Heidelberg Eyhance study) and picked up on a very interesting little tidbit… Tecnis lenses use a type of material that corrects chromatic abberation. I don't believe Alcon lenses do this. I recall reading about chromatic abberation awhile ago and if I recall correctly, different wave lengths of light (i.e. colours) travel slightly different distances. Chromatic abberation correction attempts to get all these wavelengths to converge more uniformly. This improves contrast sensitivity. So that may be a factor as well in ICBOO vs. SN60WF
.
I also think it's important when getting deep into these metrics and such to always bear in mine exactly how these tests are set up and run and most of all to remember that statistical information (results from an apparatus) and clinical information (results from actual patients) are two different things. That said I'm still leaning very heavily towards Eyhance now rather than Vivity.
RonAKA Guest
Posted
I somehow missed this response. The Alcon AcrySof material has a higher refractive index (1.55) than the Tecnis material (1.47). The advantage of the higher index is that the lens can be thinner and easier to insert. The disadvantage is that the higher refractive index material causes more chromatic abberation. It is similar to eyeglass material where the high refractive index materials have a poorer Abbe number rating. One way to reduce the impact of the light spreading is to filter out the light that spreads the most - which is at the blue end of the spectrum. I believe that is one of the reasons why Alcon use blue light filtering. It reduces the impact of the chromatic abberation light spreading. Tecnis on the other hand have avoided using blue light filtering and get high light transmission values -- even higher than a natural lens. Now they seem to have come around a bit, and offer a violet (close to blue!) filter in some lenses. This I believe is to reduce chromatic abberation. I suspect they call it violet instead of blue to try and differentiate themselves from AcrySof because they have dissed AcrySof for the blue light filtering for so many years.
I don't know what real impact this has on overall lens performance. AcrySof have claimed for years that they provide better vision at night than the clear lens options. Is it real? Perhaps we would need to get one of each in the two eyes to compare.
RonAKA Guest
Edited
I still have been mulling over the option for IOL choices for my second eye. The first eye was done corrected to plano for distance with an AcrySof IQ Aspheric monofocal lens, so at least for me that choice has been made. For the second eye I have been considering the same lens, or possibly the Vivity, but with some degree of under correction to achieve monovision. From the point of view of determining the impact on contrast sensitivity I put together a few options using data from the Alcon Package Insert from the Vivity lens. This is what the data shows without manipulation for the two lenses set for plano at distance. Contrast sensitivity is maximized for both lenses at distance. And, even though the Vivity information claims that contrast sensitivity is best when using the Vivity in both eyes, it sure appears to me that one monofocal lens and one Vivity will achieve better overall CS at distance. The upside of the monofocal + Vivity is that contrast sensitivity will be improved from -0.5 out to -2.5. So perhaps some improved reading ability in dimmer light with the Vivity eye.
.
.
The next option I have been considering is the having the Vivity eye under corrected by -0.75 D. If I understand this properly that would effectively push the contrast sensitivity curve off to the right to provide better contrast sensitivity for closer up. This graph illustrates this effect. In this case the contrast sensitivity for the Vivity lens is maximized at -0.75 and provides improved contrast sensitivity out to -3.25 defocus position. This would seem to improve reading in dimmer light even more.
.
.
And last there is the option of using the standard AcrySof IQ Aspheric monofocal with a -1.25 under correction for monovision. This graph illustrates this effect. This configuration provides a much more significant improvement in contrast sensitivity with a maximum at -1.25 and extending out to -3.0 for defocus position. I would expect overall this would provide the best reading ability in dimmer light.
.
.
This is now convincing me that using a Vivity lens for my second eye in a monovison configuration is not that great of an idea, and I am more likely to get better overall results with two monofocal lenses with the second eye under corrected to -1.25 D.
.
Comments?
Guest
Edited
Personally I'd be nervous about monovision beyond -0.75D. But that's me. And maybe you've already simulated a bigger offset with contacts and are fine with it.
.
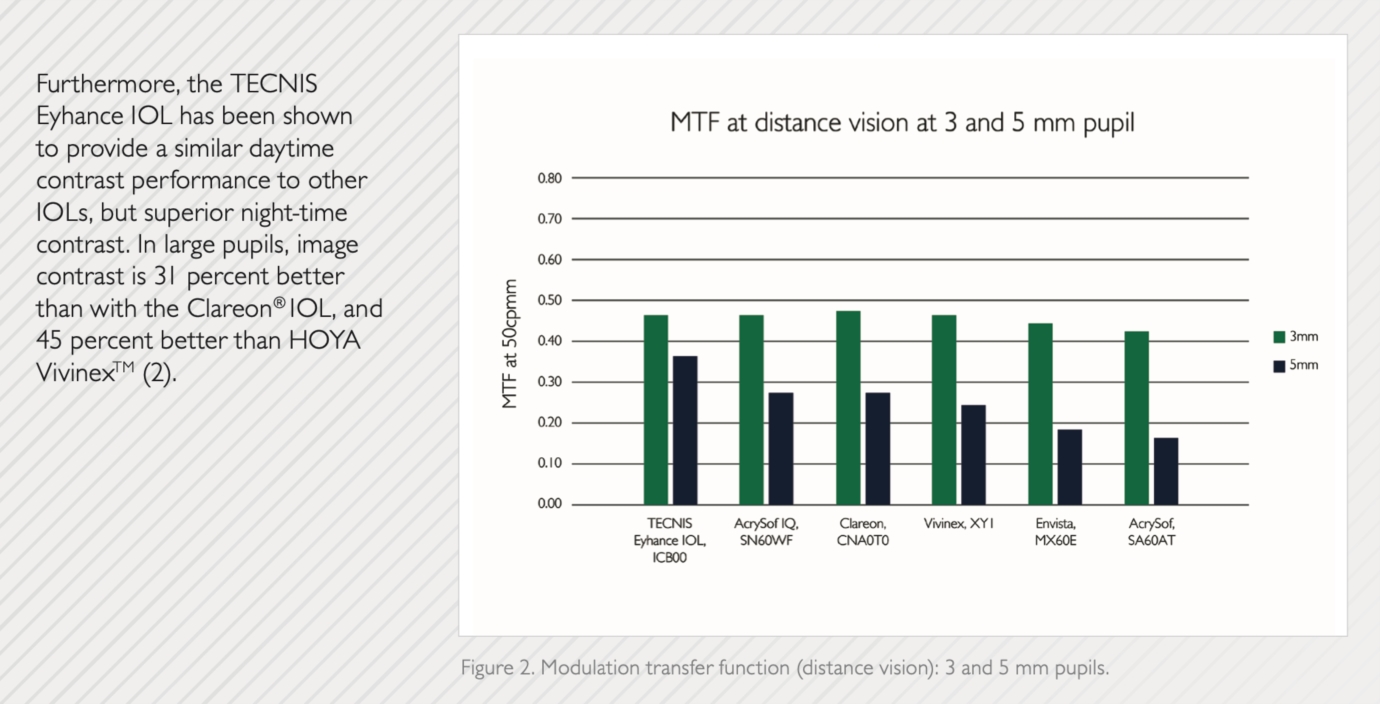
VERY interesting point about taking the defocus position into account though. I have not had any surgery yet but I've been strongly leaning towards Eyhance because of it's far superior contrast sensitivity. The MTF bench test bar graph with 3mm and 5mm model eyes from that "The Opthamologist" PDF would indicate that Eyhance has double the contrast sensitivity of Vivity. And is even better than the Acrysof Mono (presumably due to the material J&J uses which corrects for chromatic aberration).
.
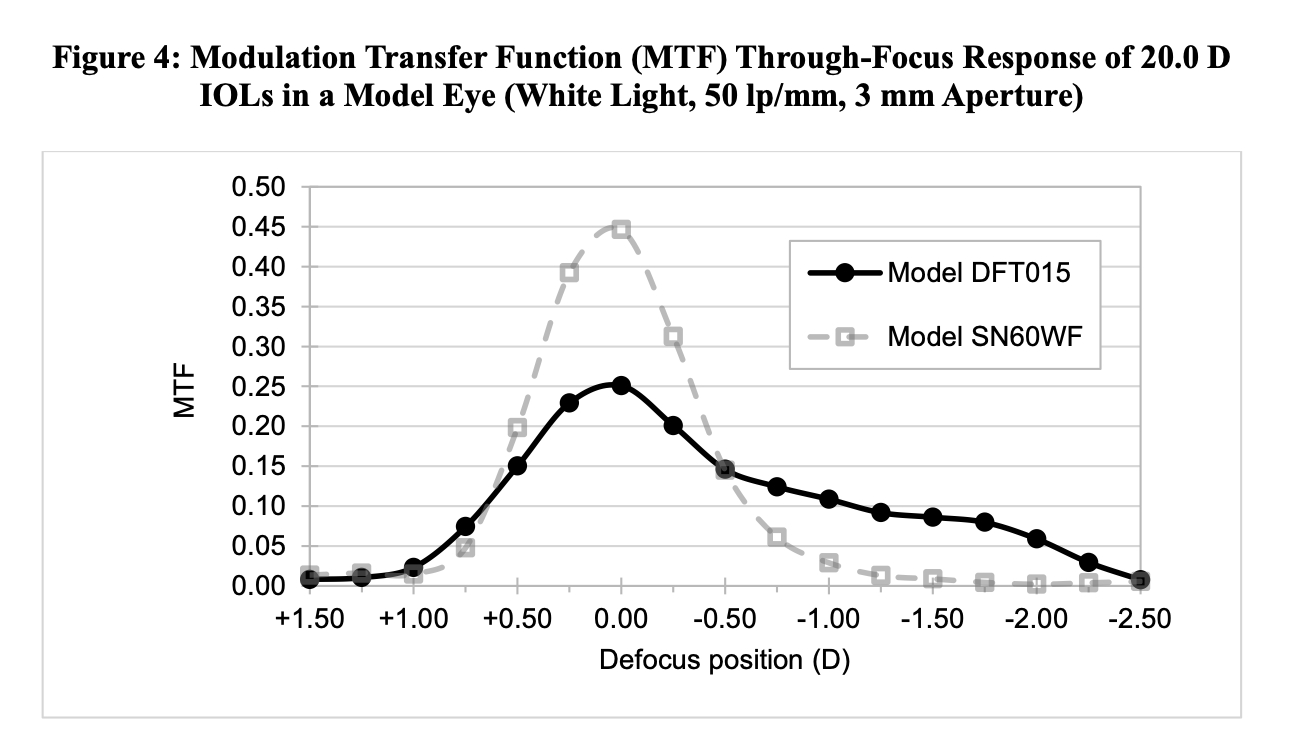
However this chart is only showing the CS at DISTANCE. So it's the PEAK CS of those lenses. I cannot find an MTF graph for Eyhance that plots the CS over a range of defocus. So I'm thinking Eyhance CS is so much better BUT... what Vivity loses in CS at distance it may make up for in CS up close. Very very interesting.
.
The only other CS data I can find for Eyhance is those clinical tests with people trying to make out charts with vertical lines in them (CPD charts). Eyhance again beats Vivity by a mile. But again those tests are probably just done in an office with normal light from 10 feet away (distance). If they did some kind of CS test with Vivity vs. Eyhance at 66cm maybe Vivity would win. I wish I could find an MTF result for Eyhance that plots CS over a range of defocus positions.
.
As for your choice, Since you had such a great result with the Acrysof Monofocal I think I'd stick with that. Keep it simple. And if you're worried about CS up close maybe do however much monovision you're comfortable with. A question for the surgeon for sure. But Vivity at -0.75D might be a good non-dominant eye choice as well.
.
But yah taking defocus into account is interesting. It's like, yes, monofocals have amazing CS but only at one single peak. To shift that peak you need glasses. Once you're trying to get yourself out of glasses there has to be some kind of trade off as you're spreading the same amount of light (and contrast) over a larger distance.
RonAKA Guest
Edited
On the amount of monofocal under correction I got a lot of useful information out of this pdf article.
.
Optimal Amount of Anisometropia for Pseudophakic Monovision Ken Hayashi, MD; Motoaki Yoshida, MD; Shin-ichi Manabe, MD; Hideyuki Hayashi, MD
It is located at semanticscholar.org
.
They determined that the optimum amount of anisometropia was -1.5 D. With contacts I tried both -1.25 and -1.5 and preferred -1.25. I also tried -2.0 D which is with no correction for me, and I don't like it at all.
.
I am pretty comfortable with -1.25 to -1.5 as a range, as I know I can't expect to get it perfect.
.
I am somewhat skeptical of some of the claims of Tecnis for contrast sensitivity. I can accept that the Eyhance may be better than the Vivity, but to say it is better than the monofocal AcrySof just makes no sense. I am also a little suspicious of them saying they do not fiddle with asphericity to achieve the EDOF. When the power of the lens varies from middle to edge that is essentially the same as asphericity to my understanding. Seems like they are playing word games to some degree.
.
It is always hard to separate marketing spin from facts!! The hearing aid companies are even worse in that respect...
Guest RonAKA
Edited
My understanding is that it's mostly down to the material used in the lens. The actual plastic they use in the Tecnis lenses corrects for chromatic aberration so longer wavelengths of light are not lost. Also the data only says Eyhance CS beats Acrysof with a 5mm "pupil" (by about 30%). They're identical at 3mm. And Acrysof filters blue light. Eyhance only filters UV. These are bench tests using the same criteria and endpoints... not subjective clinical tests... so I believe it. What I'm NOT sure about is how much it actually matters in the real world.
RonAKA Guest
Posted
Not sure. I think the only material "advantage" although there are pros and cons, is that the Tecnis material has a slightly lower refractive index. I am still strongly suspicious these tests are being influenced by the light transmission. That is a significant difference in the order of 8-10 %. The issue however is whether that is a good thing or not. The AcrySof lens with the blue light filtering attempts to match the light transmission curve of the natural lens of a young person. The Tecnis clear lens provides up to 10% more light than a natural lens. Not sure if that is good or not so good....
Guest RonAKA
Posted
yah the jury still appears to be out on that with some saying that extra "unnatural" blue light can actually be damaging. That said with literally millions of J&J lenses implanted out there I'd think any troubling signals / patterns would have emerged by now? I'm not too concerned about it but if I had to choose I would choose Alcon's blue light filtering.
RonAKA Guest
Edited
Well I did a little more research and my theory about the improved contrast sensitivity being due to increased light transmission was blown out of the water. The poorest lens from a contrast sensitivity point of view in that graph you posted was the Alcon SA60AT. Unlike the SN60WF the AT lens does not have blue light filtering. And it has much higher light transmission, but still does not achieve the increased CS. See this graph which compares the transmission for these two lenses and compares them to a natural lens.
.
.
The other difference between these two lenses is that the SN60WF is an aspherical lens to correct for the residual asphericity in the cornea, while the SA60AT is a spherical lens and provides no correction. Perhaps that is closer to the real issue.
.
On that line of thinking the Alcon aspherical lens provides -0.20 correction, while the Tecnis lens has -0.27 correction. Now I am thinking that in the simulated test method for contrast sensitivity this extra amount correction has an impact on the test results. The test method may use a +0.27 amount of corneal asphericity to simulate the average eye. It is the accepted average number for the general population. And because the Alcon lens is -0.20 it is handicapped in the test method, and gives poorer results according to the test simulation.
.
The thing that needs to be kept in mind here is that this magic +0.27 asphericity is an assumed value based on actual measurement of many people. Each eye will vary from this, and if the best correction is required, the surgeon should measure your eye and then select the best suited lens for your actual correction needed. I recall reading somewhere that this +0.27 value is somewhat skewed due to a higher portion of the world population being Asian and that Asian eyes have a higher amount of asphericity in the cornea than Caucasian people. In short if you don't have your eyes actually measured, you may be better selecting a Tecnis lens if you are Asian, and an Alcon IQ lens if you are Caucasian. Can't say I have seen the data to support that though. This is one graph I found on the distribution of asphericity in the general population.
.
.
Another theory to consider!!! I think one would have to dig deeper into how this contrast sensitivity measurement is simulated in the test to determine if this is valid or not.
Guest RonAKA
Edited
Wow lots of great info Ron. Thanks.
.
I know the bench tests (i.e. MTF) in Europe use two different artificial (model) corneas, an ISO 1 or ISO 2. The ISO 1 does not simulate corneal spherical aberration. The ISO 2 does (I think at 0.27 microns). Trials in the US use an ACE Model eye. Not sure how it differs from the ISO model eyes. Also I'm guessing tests probably can't simulate sunlight that well so the light itself may not be full spectrum. Or may favour certain spectrums. And finally a bench test doesn't have a human brain / visual cortex to make sense of the image. A human is a much better image processor.
.
The point is that a bench test is a simulation and there are lots of variables involved probably depending on who does the test and how it's setup. I think we should take those MTF charts with a grain of salt. That said if all lenses are tested on the same setup (one trial comparing them all) I think it's fair since the lenses would be the only variable. But my point is I don't know how much weight we should put in those numbers in an absolute sense. I think clinical testing is more "real world".
.
So for instance one thought I had today was, if we accept that Eyhance CS at peak focus is twice that of Vivity at peak focus (distance for both let's say) does that even matter if you're outdoors in full sunlight? Will the Eyhance patient see a better quality image because of the higher contrast sensitivity? Or is there a point at which there is SO much light entering the eye that it doesn't matter if your retina is using 50% of the light or 100% of the light? Basically if have a robust amount of light to work with is there a point at which adding more light (beyond 50%) doesn't noticeable improve the image anyway (diminishing returns). I don't know.
.
If that's the case then Vivity might be a better lens (functionally) overall because it would have more defocus CS in dim light than Eyhance (which presumably has a steeper CS drop-off at say, -1.5 defocus). Of course if you use glasses with Eyhance it will beat Vivity or any EDOF / Multifocal hands down. But we're trying to get minimize the use of glasses... so... yah.
.
Ok that was quite the ramble. Hopefully it made some sense.
.
I'm still leaning towards Eyhance for myself personally. As a myope with AMAZING glasses-free near vision it makes me nervous to know I will likely be giving that up. And it's hard for me to imagine what day-to-day life will be like without that. But if I'm unhappy with acuity / focus depth I can fix that with glasses / progressives. If I'm unhappy with image quality there's nothing I can do about that. Eyhance is less risky in terms of image quality. It's basically a Mono but with a little free bonus. I know the Vivity quality trade off is slight and probably only an issue in dim light (due to it's low CS and flatter MTF CS defocus plot) but I'm a perfectionist and I know quality issues would likely really bother me a lot. As much of a pain as glasses may be, I think I'd be better off dealing with that than dealing with a quality trade off. Even if it only manifests in dim light. But the promises of Vivity are very tempting.
RonAKA Guest
Posted
I found some old studies comparing the results of the spherical lenses to the new at the time aspheric lenses. One comment made was that age matters. The benefit of neutralizing asphericity is more of a benefit for younger people (pupil size 5 mm), and at night, than for older people with a smaller max pupil size (3 mm). They went as far as to say with a small pupil size one is unlikely to notice the difference between the two types of lenses.
RonAKA Guest
Edited
To satisfy my curiosity as to why Alcon chooses to use an aberration correction amount of -0.20 instead of the theoretically perfect (for an average eye) of -0.27 microns, I did some more research. It seems that Alcon could easily make lenses with -0.27, so I wondered why they didn't.
.
The short story that Alcon tells is that their objective was to simulate the vision of a young healthy eye. They used data from studies of eyes that produced supernormal vision of 20/15 or better. What these studies showed was that eyes with supernormal vision had a positive residual aberration of +0.1 microns, not zero. So that is their reason for targeting about 0.1 micron positive aberration.
.
They also introduced the blue light filtering to match the young eye.
.
It is summarized nicely in an Alcon article titled as follows:
.
CRSToday The Science Behind the AcrySof IQ IOL Details from one of the minds behind this aspheric IOL design. Mutlu Karakelle, PhD
Guest
Edited
I've been thinking a lot about contrast sensitivity since I realized that it varies depending on focus distance and these charts we all see are usually for peak contrast (which is typically distance vision). Contrast in any lens will drop off from it's peak with defocus. So...
.
.
The Panoptix claims to only lose 7% contrast compared to a Monofocal but do they mean across the board (all focus distances)? Or just at distance? Vivity warns of 20% or more contrast loss but I assume that's at distance. So intermediate would be worse since the Vivity MTF curve drops off from a peak and plateaus at intermediate before dropping off completely at near. So it may be ok for night driving (dim light / far focus) but you may need a light to read in a dim room (dim light / near focus)
Anyway the big question I'm wondering about is how much we should even worry about contrast sensitivity. Does decreased contrast sensitivity matter in ALL lighting conditions or mostly just in low lighting conditions? Maybe when you have more than enough light (a sunny day for instance) a 20% drop (as with Vivity) has no noticeable impact on image quality. Even though it's worse on paper. But what about distance vision when light isn't good? Snow? Rain? Fog? Glare when driving into a sunset? Night driving?
.
I guess the point is, if the lower CS of Vivity is only ever potentially noticeable in the "reading in dim light" scenario I may be putting too much emphasis on it.
RonAKA Guest
Posted
Somewhere I read that the overall vision quality is determined by the following factors in this order:
I have also read that CS is more important in dimmer light, and it is more important for those with larger pupils (probably younger people). So yes, for the typical elderly cataract candidate it may be a little over rated. It may be a bit like buying binoculars especially for good vision in lower light. 42 objective diameter x 8 power binoculars gives a exit pupil diameter of 5.25 mm (42/8). If you have pupils that size or larger this is great. However if you pupil size is 4 mm (an older person) they will provide no value for you over a 35x8 binocular which will give a pupil diameter light shaft of 35/8 or 4.4 mm. Sometimes people pay big bucks for optics that their eyes cannot really make use of.
What your research and also that I have done, has pretty much convinced me that I will not go for a Vivity lens in my near eye in mini-monovision configuration. I think I will have better overall quality vision with two monofocal lenses. The cost factor is not a big one with me, and I would not hesitate to pay more for better vision. However, it always stings a little bit to pay significantly more for a lens and come out of it with a poorer results.