Eyhance Defocus Curve and Landing Zone
Posted , 11 users are following.
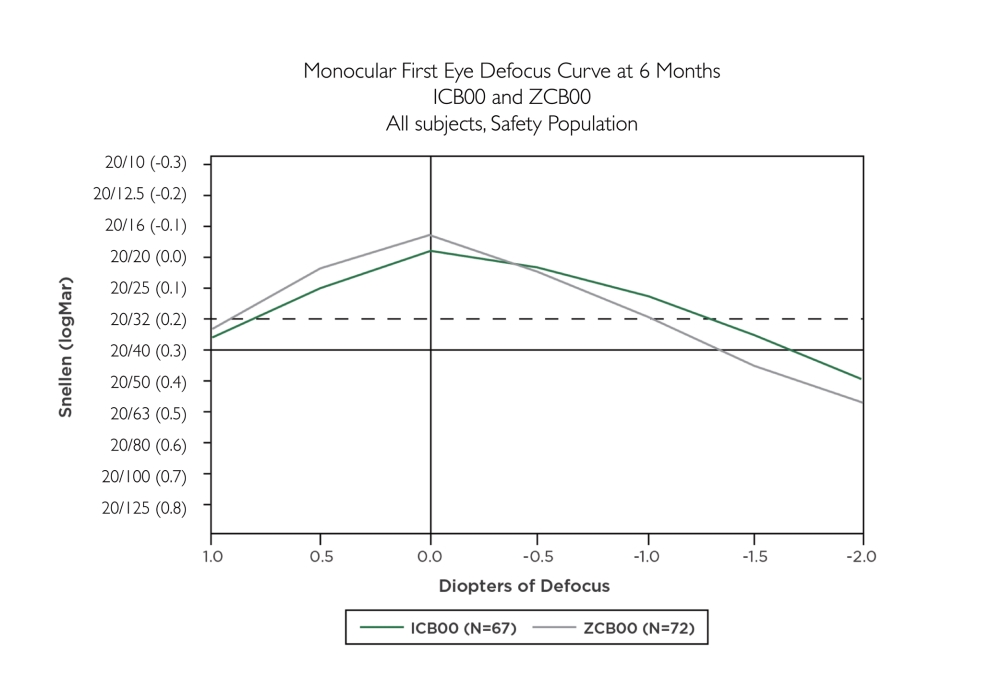
There has been some discussion of late on these issues and I came across a J&J sponsored article on the Eyhance that gives what looks like a credible comparison of the defocus curve of the monofocal Tecnis 1 (ZCB00), and the Eyhance (ICB00). This curve is below, assuming it gets posted after moderation. It shows some things that seem to get overlooked or misinterpreted in other documents. First is that at the peak, the visual acuity of the Tecnis 1 is better than the Eyhance. This makes sense as the Eyhance compromises peak acuity by using a different lens power in the middle of the lens compared to the outside. All of the light is not being focused at the same point as is done in the aspheric -0.27 Tecnis lens.
.
The other thing it shows is that the so called flatter area of the "landing zone" is to the right of the 0.0 peak acuity point, and not to the left. If the surgeon misses on the positive side acuity will not drop off just as fast as the standard monofocal. BUT, and it is a big but, if you go to the positive side you will lose near vision as the whole curve moves to the left. It does not take much of a miss on the positive side to lose all the near and intermediate vision advantage of the Eyhance. Yes, the distance vision will be less compromised, but most get the Eyhance for the closer vision it provides. In other words the surgeon is using the flat landing zone to improve their distance accuracy, but at the cost of near vision.
.
And the last thing that can be seen from these curves is that the standard monofocal Tecnis 1 provides about 1D on the plus side of LogMAR 0.2 vision (20/32), and the same on the negative side. The Eyhance provides about 0.8 D on the plus side and 1.3 D on the negative. It is barely more than the standard monofocal for total depth. The important side of course is the negative side and it provides about 0.3 D extra depth of focus. This falls short of the minimum standard for an EDOF which is an extra 0.5 D. It does indicate that the Eyhance suffers more loss of distance vision when you under correct in a monovision configuration.
.
.
You should be able to find the complete article by googling this:
.
Delivering Intermediate Vision: The New TECNIS Eyhance Monofocal IOL Highlights from the Frankfurt January 2019 Advisory Board Meeting
1 like, 100 replies
billy111 RonAKA
Posted
Ron
That was a excellent technical analysis of the Tecnis 1 ZCBOO. You are extremely knowledgeable about optical physics.
Myope_PSC RonAKA
Edited
That's a monocular curve chart so only one eye. Both the ZCB00 and the ICB00 exceed 20/20 monocularly based on the average of all those single eye outcomes in the study. That's good.
That should average out to 20/16 or better when binocular summation kicks in for those that target distance vision in both eyes. That's great.
For folks interested in monovision, they should be made aware that they don't get all those benefits.
Those quoted paragraphs are from Jack T. Holladay's "Should I choose distance vision in both eyes, monovision, EDOFs or multifocals?" for anyone interested in learning more.
Residual astigmatism needs to be considered when choosing targets in my opinion. Spherical Equivalent (SE) is calculated by adding half of the cylinder to the sphere refraction result. For those that want good distance vision, I'd be wary of targeting too far away from plano when residual astigmatism is expected.
Examples of residual astigmatism with different sphere outcomes with near plano target:
+0.50 sph, -0.75 cyl = SE +0.125
-0.50 sph, -0.75 cyl = SE -0.875
From those examples I'm sure that the SE +0.125 eye would have much better distance vision than the SE -0.875 eye.
jimluck RonAKA
Edited
"It does not take much of a miss on the positive side to lose all the near and intermediate vision advantage of the Eyhance." --RonAKA
I interpret it differently. If the surgeon misses to the positive side, the Eyhance still retains the same advantage over the monofocal. Both curves shift the left, so at any given point in the near and intermediate ranges the Eyhance curve still lies above the monofocal, albeit both are lower due to the miss.
greg59 jimluck
Posted
I think Ron is right, especially in lower light situations where the Eyhance curve shifts left while the monofocal curve stays in place. Target plano with Eyhance and you'll likely be even less happy in low light than if you'd chosen a monofocal. All the intermediate/near vision advantage of the Eyhance goes away in low light as the pupil enlarges and uses more of the higher-powered lens periphery.
RonAKA jimluck
Posted
I think there is more temptation for the surgeon to miss on the positive side with the Eyhance. They know distance vision will not be compromised as much due to the flatter curve. The temptation for the monofocal is to miss on the negative side so closer vision is not compromised. Common for surgeons to target -0.25 with a monofocal. I recall I have seen some surgeons claiming they target the Eyhance to be positive.
greg59 RonAKA
Edited
The larger the pupil, the more power on the periphery of the lens you'll have available for distance vision with Eyhance. This creates a hyperopic shift in the defocus curve for pupils larger than the relatively small pupils used to create the curve. Myope_PSC has referenced articles that show a shift of 0.5D in the hyperopic direction for relatively modest increases in pupil size. Monofocals do not have this property.
When you describe Eyhance, pupil size is a huge factor that doesn't affect other lens designs. Shift Ron's curves to the left by 0.5D and you'll get an idea of what you'll see in low light or at dusk. When it's dark, you may need to shift more than that.
If your the optimal Eyhance lens acuity is set at -1D (focus at 1 meter) then you should see about 20/30 at distance according to Ron's curve. With that relatively bright light, the curve suggests that you'll have 20/32 vision down to about 16 inches. Functional 20/40 phone vision could be had at 14 inches. Individual results will vary but dim those lights just a bit and the enlarged pupils will use more of the powerful outside of the lens and you'll see at about 20/20 at distance. However, your intermediate and near vision will fall off quickly as the outside of the lens isn't much help at near.
Targeting plano with the Eyhance will only help intermediate/near vision in bright light or with small pupils. Once the pupil gets large enough to use the more powerful outside of the lens, the defocus curve shifts left and the intermediate/near vision becomes similar to the monofocal if not worse.
I spend most of my time in environments where I have little or no control of the lighting. Unfortunately, most places are relatively dim and I need the best near and intermediate vision possible in these environments. Targeting anything close to plano would leave me constantly putting readers on and off, assuming I could find them. That's why I chose to target my lenses at -1D (achieved 0.9D) and -1.3D. Just had the 2nd lens inserted today so I'll see how it works when I take the patch off.
With completely dilated pupil in outdoor shade, even with the clear plastic patch I can see far better looking 30 degrees away from where my head is pointing rather than through the middle of the lens. That illustrates Ron's point about the outer portions of the Eyhance being more powerful than the middle. It also supports the hyperopic shift with increasing pupil size theory.
Targeting intermediate (say, -1.25D) gives you great night distance vision, good distance vision on cloudy days or at dusk, and barely drivable distance vision driving into bright sunlight or when pupils are small. You should be able to see at intermediate well, even in reasonably dim light. Near vision will be great in bright light but will decline with decreasing light even faster than a monofocal. But you can't get this overall vision profile with a monofocal no matter where you target it because it's defocus curve doesn't shift with pupil size.
Contrast that with targeting plano where you get great distance vision in bright light and become significantly hyperopic in lower lighting or at dark. That might give you 20/15 or 20/10 distance vision but shift far enough in the hyperopic direction and vision will decline. Intermediate/near vision will be as advertised in bright light but will essentially disappear in moderate / low light.
If you can control the lighting in your environment, targeting plano might be a good choice. If you need intermediate/near vision in poorly lit spaces, I'd recommend targeting intermediate, avoiding hyperopic surprise and relying on the shifting defocus curve to provide decent distance vision in less than optimal light.
Myope_PSC greg59
Posted
I don't think most people will end up with great night distance vision or good distance vision on cloudy days if they end up around -1.25D. I say that based solely on my experience so I could be wrong.
For those of us that choose distance as the target for both eyes with monofocals, we're already expecting (or should be expecting) to need glasses or other correction for actual near vision and low light intermediate vision needs.
If someone ends up at plano or very near plano on the minus side then a small hyperopic shift when it's dark will make night driving better and small myopic shift when it's bright might go unnoticed if they remain at a good 20/20 throughout. I've mentioned the shifts and Greg has also but no one else on the forum has as far as I know.
Greg - Do you have an eyeglasses prescription at this point or is it still too soon for that? I'll be interested to find out if your thoughts on all this change with refraction results.
RonAKA greg59
Posted
It seems to me that monofocal IOLs are significantly impacted by light level as well. With my near eye Clareon IOL I can easily read J1 at the prescribed 14". However in more normal indoor lighting it is closer to J3. This eye is kind of messed up with astigmatism, but on a spherical equivalent basis it is around -1.5 D. Without our accommodation ability in the lens we become much more dependent on the small pupil pinhole effect and the associated depth of focus improvement.
RonAKA Myope_PSC
Posted
One comment I saw somewhere about the Eyhance and eyeglass prescription is that the autorefractor instrument tends not to be accurate. And also when determining the prescription with a phoropter that there should be some bias toward the plus side.
greg59 Myope_PSC
Edited
I haven't used prescription glasses since my first lens was replaced 5 weeks ago with a -0.9D focused IOL. I can read books when the lighting is excellent but near vision declines quickly as the lighting gets dim. I struggled in low light with computer monitors but could hold my natural -5D eye close enough when necessary. I haven't had any problems driving, even in bright sun when my distance vision is at its worst.
I lost the option of using my -5D near eye yesterday when I had the 2nd lens replaced. It'll be another six weeks or so before my eyes have settled enough for an eyeglass prescription but I'm not sure I'll need anything except for close up and pill bottles. I think I'll be 20/30 at distance in the brightest sunlight but 20/20ish any time my pupil gets large enough to take advantage of the more powerful lens periphery. Thought about getting prescription sunglasses but high quality non-prescription sunglasses might keep the pupil large enough to improve bright-light distance vision to near 20/20.
We targeted -1.3D (30 inches / 77cm focal point) for the second eye yesterday and today I'm already seeing quite well at distance with that eye - close to 20/20. I don't know if the target was achieved. My pupil is still somewhat enlarged from the surgery so I'm getting "enhanced" distance vision (and poor near vision) despite being in good lighting. Intermediate vision is decent...I can read this screen from about 30 inches in good lighting (but it's not quite as sharp as with my other IOL). When my pupil gets smaller (hopefully by tomorrow) I'm expecting my distance vision to decline a bit in good lighting but still be strong in low light. Near vision should improve with the smaller pupil.
My binocular vision is starting to improve with the 2nd IOL (I haven't had any for at least 2 years).
Even though I had no expectation of being "spectacle independent", I think I'll be about as close as one can get with the Eyhance. Distance vision is already better than good enough to drive in all lighting conditions. The real test will be next week when I go to the dimly lit computer lab where I teach and see if I can read student screens. If I can, I wouldn't have to carry around readers - just have some in the kitchen to read pill bottles and small print on packages. If not, I'd get some high quality prescription readers or progressives to wear at work.
jimluck greg59
Posted
I am surprised room lighting affects your ability to read a monitor. The monitor is its own light source. Can you help me understand why that's an issue for you? I'll try it myself tonight.
greg59 jimluck
Posted
My problem in the lab may be that my pupil can't react quickly enough. I'll be speaking to students in dim lighting, pupil a bit larger than normal. Then I quickly glance at a screen and expect to read - immediately. I'm not constantly staring at the monitor - just occasionally for less than 1 minute. I'm not sure my pupil is getting the right signals to immediately reduce diameter (or if it could immediately reduce size if it wanted). Some screens have dark fonts on white backgrounds, others have light fonts on dark backgrounds. Dark backgrounds wouldn't send signals for the pupil to reduce size. Still, younger people don't seem to have problems with this task.
RonAKA jimluck
Posted
I don't notice this issue of room lighting changing things much when using a 24" monitor. However when watching a 65" TV from 8 feet or so, I find things improve if the room lighting is on, compared to it being dark around the TV screen. I suspect the room lighting causes my pupils to constrict more, which sharpens up the image.
RonAKA greg59
Posted
"younger people don't seem to have problems with this task"
The young folk with natural lenses have a functional accommodation system working for them.
jimluck greg59
Edited
I am soon to be 73. My pupils are always tiny now, unless dilated with drops. I have good corrected night vision despite epiretinal membranes and moderate cataracts. Seeing a monitor in darkness is not challenging for me if I get the focal length right and the font is not too tiny. I wonder if your issue is something else.
I wonder if my always-tiny pupils will be better for Eyhance. I think it's an old-age thing.
let's see if this works (pupils closeup selfie in dim light)
RonAKA jimluck
Posted
Small pupils are helpful with monovision. I suspect they increase the depth of focus. I recall that one study I read was that monofocals in both eyes using monovision works well if pupils are small. But, with younger people and larger pupils hybrid monovision is better with an EDOF in the near eye. Distance eye in this study were for full distance vision.
greg59 jimluck
Posted
I'd guess that you wouldn't get as much benefit from the periphery of the Eyhance as I do at distance in low light or at night. My pupils still dilate fairly well. Old-age usually reduces pupil function and I've wondered if I'll retain benefits of the hyperopic shift as my pupils get smaller.
jimluck greg59
Edited
Correction: I did some experiments using my computer monitor, a webcam and a bright light in a dark room (I didn't have a mirror handy). My pupils do get big in darkness but they get small again really really quickly when I turn on the light so I was not seeing the large-pupil phase. I had no idea the change was that fast. Cool!
Spoo greg59
Posted
Greg, you mentioned that you were seeing better tilting your head 30 degrees, is that a constant thing with the Eyhance or only in some circumstances / bright light. Are you pupils overall pretty small to begin with? I'm trying to figure out if my 4.3 millimeter pupils would have this issue because it will certainly be bothersome to me.