Fitting range of AcrySof IQ Toric IOL
Posted , 3 users are following.
Hi, I'm 70 years old and getting prepared for my first cataract surgery pre-op appointment. And, I am trying to get up to speed on what my choices might be for a replacement lens. Over the years my eyeglass prescriptions for this eye have been in the -3 to -4 range with astigmatism for the last 20 years or so (as best I can remember. And for a long time I have been getting a +2.5 add for reading. I have used contacts on and off, and have more recently mainly been using progressives. Here are some old as well as the more recent corrections, which indicate my eyes have been changing and actually getting significantly better for distance, up until very recently with the cataract diagnosis.
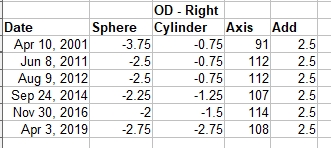
My initial investigations have led me towards a distance distance only toric solution. My first priority is image quality and I am not against wearing glasses. And, I will have to anyway until my second eye is done. I have close to 20/20 in it now, so I don't know how far in the future that will be.
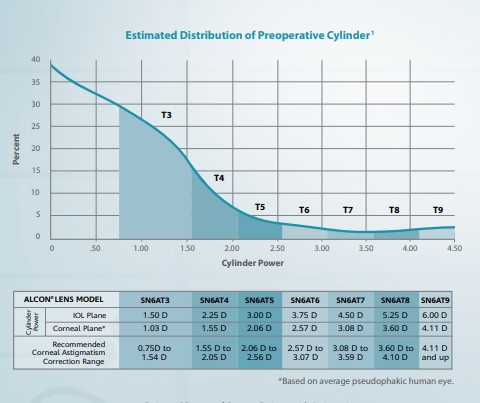
So my question is about whether or not these AcrySof IQ Toric IOL's are suitable. Does it look like my correction needs can be accommodated by these lenses? This is what I see from one reference I found for this.
I am thinking that my last prescription which was made to try and correct for the mess the cataract has made, has to be ignored, and my needs are more based on what I had before the cataract came into the picture. Thoughts?
Moderator comment: I have removed the link(s) directing to site(s) unsuitable for inclusion in the forums. If users want this information please use the Private Message service to request the details.
0 likes, 16 replies
RonAKA
Posted
"Moderator comment: I have removed the link(s) directing to site(s) unsuitable for inclusion in the forums. If users want this information please use the Private Message service to request the details."
I am new to this forum. What kind of links are unsuitable for inclusion in a post, and what are suitable?
RonAKA
Posted
Perhaps I should have asked my question in a simpler way. Is there any rule of thumb way to predict IOL plane spherical and cylindrical power based on eyeglass prescription powers?
Guest RonAKA
Posted
I believe your eyeglasses are made to suit the power from your natural lens, which you remove during cataracts surgery. So I would say no, those numbers from the glasses are not useful.
Iols are made in a very wide range, because people are very different.
My iols have a power of 29.5 both eyes, which is considered a high number, I think a measurement for glasses before surgery would have been somewhere around +2.
The surgeon will make precise measurements before deciding the right lens for you.
RonAKA Guest
Posted
Thank you for the response. I know the doctor is the one that will decide what power I need, and I really don't need to worry about it. What I was mainly trying to do is get prepared for what options are likely to be made available to me so I can make an informed decision when the time comes. About all I have been able to figure out from on line information is that about 60% of our focusing power comes from the cornea shape, and the remainder from the shape of the lens. And I guess there is no way of really determining which of those two is responsible for our vision loss without actually measuring the shape of the cornea.
What I am concerned about with the AcrySoft IQ Toric lens is that with the fitting ranges they provide, I may between the AT3 and AT4 type, and not be suitable for either?
Guest RonAKA
Posted
I fully understand your worries, we are all worried about the choice we are making before surgery. And some, including myself, also had some time after surgery where I questioned my choice, thinking what I might could have had instead.
Fact is, that the theoretical perfect is never achieved in real life, but most of us gets really good results.
All surgeon have some lenses they prefer, and they use them thousands of times each year, and they learn how to make the best possible outcome, with the stuff they are using.
I don´t have Acrysof lenses myself, I have Zeiss, so I don´t know about AT3 and AT4, I am guessing it maybe have something to do with the astigmatism?
Astigmatism can be caused and cured in different ways, some surgeons prefer to fix mild astigmatism with some "relaxing" cuts with the laser of the cornea, or they can touch up and correct the remaining astigmatism this way, if the toric lens did not hit the precise target.
I have toric lenses both eyes, astigmatism have reduced from 3.0 to 0.25 both eyes, which I think is a really good result, so I would recommend toric lenses any day, if your surgeon finds you to be a good candidate.
I am sure your surgeon will pick the right lens for you, and you will have a good result, these guys/girls are pretty good at what they do 😃
RonAKA Guest
Posted
The research I found basically suggested that the best method to reduce astigmatism is with a toric lens. A second choice is to use the relaxing cuts. In any case 0.25 that you have is about as close to zero as you can get. Some even argue that some astigmatism is preferred to give you a wider range of focus. Not sure I buy that one though.
RonAKA
Posted
I apologize for this question as I was misreading this chart from Alcon. I thought each of the 7 types was specifying spherical power as well as cylindrical power. It is only cylindrical correct for astigmatism. Independently the lenses are available in 0.5 increments over a very wide range. My loss will certainly be within the fitting range, except for the possibility my astigmatism may be at the lower end of the range that is recommended for correction. So, that is now my new worry? No end of them!
In any case I found a good article called "Astigmatism: How Low Can You Go?" in the October 2018 issue of Review of Ophthalmology. My conclusion is that with cost no object reducing astigmatism to as close to zero as possible is a worthy objective for best vision. Will have to see how I measure up to see if the AT3 lens is going to be too much or not.
RonAKA
Posted
One of the things I have found in my research is that the correction needed in an IOL can often be surprising. One situation that apparently happens is that astigmatism in the cornea may be corrected out to some degree by astigmatism in the lens at a different angle. Then when the lens is removed the full astigmatism in the cornea is revealed and the IOL has to correct for more than what eyeglasses would have to correct for. I guess the bottom line here is that the shape of the cornea is what determines the IOL power required, and that will only be known when the cornea shape is measured.
ara21947 RonAKA
Posted
I still have some astigmatism despite $4000 for toric lens. Its less astigmatism than before. Some of it supposedly helped get my near vision where I wanted. My optician shrugged telling me you still have astigmatism and that he sometimes wonders if toric lenses are a money maker 😦
I definitely see better and clearer now with toric implants but my glasses for distance will still have some correction; I noticed also during the eye exam those dotted holders against the eye made things even clearer. With time, IOLs may get better and surgery improve. After all, what's with so many of us developing PCO after surgery? Patient for life after this procedure I guess.
RonAKA ara21947
Posted
I had the paddle with the holes in used to see if it would improve my cataract vision. It did. I took that to be a quick and dirty method of determining if vision could be improved with a refractive lens, without going through the optometrist trial and error method with actual lenses. Just my guess...
ara21947 RonAKA
Posted
it means you have astigmatism basically. We squint and see better or we look through pinholes to see better reducing the light scatter onto our astigmatic eyes. You cant read a certain line without the assist of correction of your astigmatism in the eyechart. How much correction is done is the surgeons decision.
RonAKA ara21947
Posted
I have had myopia for 60 years. I have always been able to see better by squinting or looking through a small hole. It is only in the last 15 years or so that I have had astigmatism significant enough to correct.
Guest ara21947
Posted
Astigmatism can be a bit of a joker, but toric lenses are not just a money maker 😃
I have toric lenses both eyes 3.0, and astigmatism was reduced to 0.25 both eyes, which is a really good result.
Pco is your body trying to replace the tissue that have been removed, so pco is very natural. When you are having iols put in, the surgeon makes a hole in the front part of the capsular bag, otherwise pco would happen on the front part as well.
But the surgeon leaves the back side of the capsular bag intact, because it is more risky to open up the back side of the capsular bag with the vitreous gel that are right behind the capsular bag. We want the iol to settle first, and then when pco becomes a problem, the surgeon makes a hole in the backside of the capsular bag as well with yag laser.
So pco really are not caused by faulty iols, it is your body that respond to the trauma, but it would be too risky to make a hole in the backside of the capsular bag during implant of the iol.
Not that many years ago we did not have iols, back then the cloudy lens was removed, and people got really thick heavy glasses. Personally I am very thankful that science have come such a long way, and has giving us the iols we have today, even that there is still room for improvement 😃
ara21947 Guest
Posted
Ofcourse its wonderful what the IOLs can do. It was my optician with his years of experience who wondered about toric lenses and how many are now getting them. He did say I couldnt have gotten any closer vision without compromising the distance so he felt my surgeon did an excellent job. I was just surprised that at only 1 month post surgery I'm already being told I'll eventually need yag correction for PCO already mildly present in the left eye. The one he sutured so tightly my eye pressure zoomed to 36. (I was then told this was a good thing since my implant wont rotate!) I think more work needs to be done by all these companies/ surgeons making so much money to improve this. We dont look at other surgical implants and say in 6 months we need to correct the inevitable scar tissue. I believe in a few years this additional laser procedure may not be needed so frequently as they learn more and more.
RonAKA ara21947
Posted
"After all, what's with so many of us developing PCO after surgery? Patient for life after this procedure I guess."
My surgeon has given me a choice of AcrySof or Tecnis aspherical monovision lenses. One of the things I have found in my research is that there is some indication that the material, and edge shape of the AcrySof lens may have advantages in the reduction of PCO. If you Google the following you should find the report, which is really just a compilation of the findings of a number of studies.
Effect of AcrySof versus other intraocular lens properties on the risk of Nd:YAG capsulotomy after cataract surgery: A systematic literature review and network meta-analysis
RonAKA
Posted
I should have mentioned that this study was funded by Alcon, the manufacturer of AcrySoft lenses, so keep that in mind if you read it. I don't dismiss manufactured sponsored studies as we would not have new prescription medications if that practice was not allowed. And I don't think they are always bias. My thoughts are that they are bias in the fact that they exist. I suspect that many studies are done by the manufacturer of a product or drug that never see the light of day. In other words the bias is in whether or not they are actually published. This one turned out positive for Alcon, so it got published!