IOL Power Calculation Formulas
Posted , 9 users are following.
Although most surgeons do not share the information with patients unless asked, they all have to measure your eye with instruments like the IOLMaster 700, Lenstar LS-900, and Pentacam. Then they use those measurements to calculate an IOL power that will achieve the target refraction in each eye. These measurements and calculation results are summarized on an IOL Power Calculation datasheet. If you ask the surgeon for this datasheet you can do your own calculations if you are so interested. This link is to an article that explains the numbers on the datasheet from the IOLMaster.
.
Do all formulas give the same results? No, they do not, and there will always be a range of results. If the best formulas agree on the correct power, then you can be pretty confident the power will achieve the predicted results. But, there is always some risk, especially for the first eye to be done. A recent study ranked the accuracy of the various formulas with 4 of them having over 90% chance of being within +/- 0.5 D of the predicted result. In this study the Artificial Intelligence based Hill-RBF 3.0 came out on top at 95%. Here is a graph of the results, and a link to the article it came from.
.
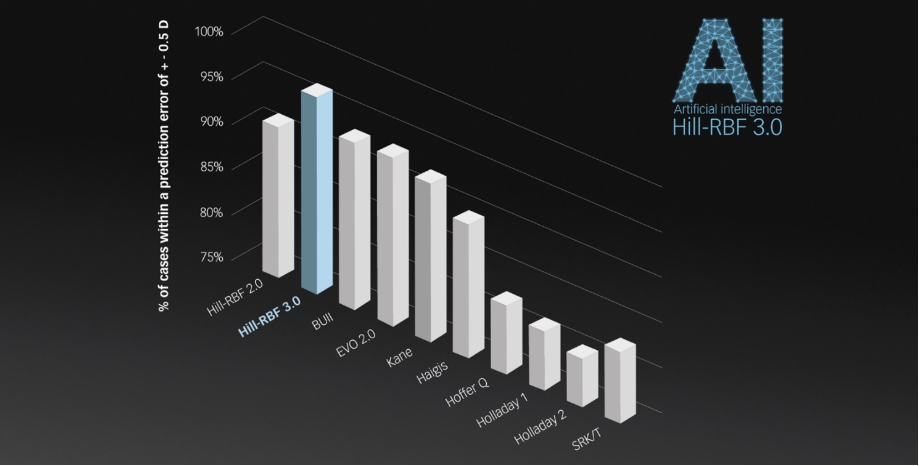
https://eyewire.news/news/study-shows-highest-iol-prediction-accuracy-for-hill-rbf-30
.
The top formulas can be found at these links:
.
Hill-RBF 3.0
https://rbfcalculator.com/online/index.html
.
Barrett Universal II
https://calc.apacrs.org/barrett_universal2105/
.
EVO 2.0
https://www.evoiolcalculator.com/calculator.aspx
.
Kane Formula
https://www.iolformula.com/agreement/
.
Note that these formulas are for non toric lenses, although the Barrett Toric formula can be found on line. They make predictions on a spherical equivalent (SE) basis which is sphere plus 50% of cylinder. Normally a target is set based on a spherical equivalent basis.
.
These formulas are most valuable on the second eye to be done as you will know what the outcome refraction is for the first eye after you get tested at 5-6 weeks. This will show which formula is most accurate for you, and you can have even more confidence with that formula for the second eye.
2 likes, 16 replies
Dapperdan7 RonAKA
Posted
thanks ron. so if one is getting a toric iol, will the spherical equivalent number likely decrease to less or zero depending on if its corneal or lens versions of astigmatism ?
RonAKA Dapperdan7
Edited
The IOL Power calculation only considers corneal astigmatism as the natural lens is gone after cataract surgery. So your starting point is only predicted corneal astigmatism, and typically it is not corrected unless it is predicted to be more than -0.75 D.
.
That is why one cannot make any firm decisions about the potential for post surgery astigmatism, or need for a toric lens until after the detailed measurements are taken for the eye. Without those measurements you will not know what the corneal astigmatism is.
Dapperdan7 RonAKA
Posted
ahh that makes perfect sense.
thank you
judith93585 RonAKA
Posted
Very interesting!
sam36130 RonAKA
Posted
hi Ron, my surgeon told me he uses -0.2 as the target for monofocal distance. is that possible? if target is missed, having residue myopic might be ok since i am a high myope. what if it went the more positive direction? how will i see?
thanks!
RonAKA sam36130
Posted
A target, is just that, only a nominal target. If you look at that first Zeiss link that I posted and in particular on page 5. Then look at the right hand OS Left eye side. Nearer the bottom under the Barrett Universal II heading (a formula), you will see a column of potential powers of IOLs that could be used for this particular eye. While IOLs come in 0.5 D steps, eyes do not. Each eye is different. So the predicted outcome of each power is displayed in to the right of the power. In this particular case a +11.75 D lens is predicted to give a -0.05 D outcome which is real close to a perfect plano (0.00 D) outcome. However in this situation most surgeons will instead select the +12.0 D power lens which is predicted to give an outcome of -0.22 D.
.
Why do they do this when the objective is distance vision? Well, this is just a prediction and they are doing well to hit this number. If it instead turns out to be +0.25 D which is being far sighted then it impacts distance vision a small amount, but at the same time it reduces the nearer vision. So, the common practice is to target a small amount of myopia in the -0.25 D range, instead of targeting a perfect plano outcome. It is try and avoid leaving you far sighted.
RonAKA
Edited
While these general formulas may work well with most eyes, those who have had previous refractive surgery like @phil09 may want to be a little more selective with the instrument used to measure the eyes, and the formula used calculate the correct IOL power. The article at the link may be helpful. Later versions of the IOLMaster 700 instrument can not only measure the anterior (front) side of the cornea, but also the posterior (back) side. Less advanced instruments don't measure the back side and only estimate it. They call it Total Keratometry or TK. I gather that the posterior surface is less affected by the Lasik or PRK incisions and can give a more accurate prediction of what the effective power contour of the cornea really is. When combined with a formula specifically designed for eyes with prior refractive surgery that uses TK better accuracy can be achieved. You can read this article to get all the details but it looks to me that it would be worthwhile to find a surgeon that has the latest IOLMaster 700 with the Barrett suite of formulas. It would appear the top pick may be the Barrett True-K TK formula, but there are other choices which are close like the EVO TK. It may be worthwhile to see the predictions of each, when making a final decision on the power to use for the best accuracy.
.
https://www.zeiss.com/content/dam/med/ref_international/products/optical-biometers/iolmaster-700/documents/iolmaster-700-tk-compendium-en-32-010-0061vi.pdf
Dapperdan7 RonAKA
Posted
do the three instruments you mentioned all cover the same needed measurements?
RonAKA Dapperdan7
Edited
Yes, more or less. I think the latest IOLMaster 700 is the best. It measures both sides of the cornea surface (TK), whereas I am not the Lenstar LS-900 or the Alcon Argos do. TK is not essential but it can give more accurate predictions of power in someone that has had prior Lasik surgery, especially when a formula is used that takes the TK measurements.
RonAKA
Edited
When looking for something else I stumbled onto this ESCRS IOL Calculator site at this link:
.
ESCRS IOL Calculator
.
It is very useful in that it calculates predictions based on up to 7 of the most modern IOL calculation formulas. It then displays the results in a table of values with the recommended power from each formula highlighted. Data only needs to be entered one time. If you are considering different targets or different IOL lens models you just edit that portion and recalculate. When you pick the brand and model of your specific IOL it enters what it believes is the best A-Constants for each formula automatically. It can be over ridden if you want to use a custom A- Constant.
.
Limitations:
.
Hope that is helpful for those debating over what power of lens is best for them. Based on the numbers I see coming out of this the Hill-RBF seems to the latest Hill-RBF 3.0 formula. All around that is probably the most accurate one there, but it can establish some more confidence if comparable results come from other modern well respected formulas like Barrett, Kane, and EVO.
karin08666 RonAKA
Posted
Good find Ron. I decided to enter my calculations just to see what the different IOL formulations would say. The Hill-RBF and the Barrett were right on with what my surgeon chose. It was interesting to see how different the other ones were. I also tried different lenses and found it very interesting that the IOL "power" would have been different. Alcon for example, would have been .5D less in each eye.
RonAKA karin08666
Posted
But, how did the formulas compare to your actual outcome with each eye? That is the critical part. If you do this after the first eye has healed then you can pick the best formula for the second eye based on which one was most accurate on the first eye.
karin08666 RonAKA
Posted
I had my left eye done first and he chose 20 D IOL with a target of -0.10 D for the eye. My left eye's outcome is -0.125 SE, so pretty much right on. My right eye was done second and the IOL was 21 D and the target was -0.55. My right eye ended up at -0.75 SE, so well within the targeted range.
RonAKA karin08666
Posted
Yes, that is good accuracy eyeglass refraction of sphere and cylinder is made in 0.25 D steps. It is possible your SE is somewhere between -0.5 D and -0.75 D.
stuart86579 RonAKA
Posted
I've just had surgery to correct Left eye +2.00 and Right eye +4.00 for distance vision. The IOLs implanted were Left +26.0D and Right +27.5D. Eyhance monofocal.
Does that sound about right?
RonAKA stuart86579
Posted
The IOL powers you need depend on your eye measurements. But, in general that looks to be in the ballpark. IOL powers above about +19.0 D are used to correct someone that is far sighted. The more far sighted you are, the higher the IOL power needed to correct back to plano. The real test of course is to get an eyeglass refraction test at 5 weeks post surgery when the eye has healed from the surgery. That is the measure of accuracy achieved.