MonoFocus For distance help needed surgery in two days. Choices????
Posted , 8 users are following.
Male, 65 years old, developed cataracts over time, I had been farsighted only needing glasses for reading over the last 15 years, prior to that good vision all around.
Last couple of years, my vision has shifted to near sighted and distance has become blurry, especially inside , low light and especially at night, Can no longer drive safely at night. So I am now near sighted.
Going to top rated practice near me, St Lukes Cataract & Laser institute. During the initial consult, they recommended Panoptix multi focus as my best option, and never really discussed pros and cons of other options. They advised me that with Panoptix, only a very small percentage have the halo and other problems that are associated with this type of lens and they will laser correct for free to improve if needed. Made it seem so simple.
They do not recommend mono vision and if I elect mono focus, they recommend only set for distance. They also offered Vivity but advised not as strong near vision( so why offer it?) They basically said make a decision without any info on what it means, giving me 2 brochures for the upgrades only, that are basically company marketing materials
After my own research and thanks to this site, I have decided on mono focus set to distance, I think. I find it hard to find good information on exactly at what distance I won't need glasses.
I know it's a combination of surgical skill, luck and eye configuration, but at less then arms length, will it be impossible to see anything clear, or is it more subtle ?
Since I am now near sighted, If I get the mono focus for distance, I will temporarily have mono vision. Can I rely on that to tell me how well I can adjust to mono vision in the 2 weeks before the next eye is operated on? Or should I wait longer. My right eye is dominant and they are doing that one first.
Any advice is greatly appreciated.
0 likes, 11 replies
RonAKA Pifutoast
Edited
My issues were somewhat similar to yours except that in my younger years I was about -4.5 near sighted. Over time as I was losing my close vision and needed progressive glasses my vision improved for distance to about -2.00 with some astigmatism. Then the cataract came in one eye. The first thing I noticed was double vision in one eye and after I noticed that I also realized the vision in that eye was blurry too. Went on the wait list for cataract surgery.
.
At the initial consult the surgeon who is a teaching professor at the University of Alberta suggested a distance lens. His frank advice was that he has difficulty recommending a multi focal lens like the PanOptix to his patients because he would not put that lens in his own eyes. That combined with the advice from a friend that was disappointed in her PanOptix lenses ended that as an option for me. The surgeon was recommending the Alcon AcrySof IQ Aspherical lens, but also offered to use the Tecnis ZCB800 monofocal lens. I chose the AcrySof and have had it in about 6 months now. Other eye is still not bad enough to do yet.
.
My bad eye was my right one and my left eye is dominant. Had a discussion with the surgeon about correcting it for distance and what implications that would have on monovision when it came time for the second eye. He said that while it is normal to do the dominant eye for distance, he has not seen anyone have trouble with doing it the other way. It is called crossed monovision. His preference was to do the first eye for distance and see what the outcome was before deciding on the second eye. I went with his recommendation, as I am a shooter and would prefer that my right eye was corrected for distance (right handed). This said I think it is preferable to have the dominant eye corrected for distance.
.
Had my vision checked for eyeglass prescription at 6 weeks and it was 0.0 D spherical and - 0.75 cylinder. Prior to surgery this eye had much more astigmatism, but the surgeon's measurements of the cornea indicated there was between 0 and 0.4 astigmatism. Astigmatism from the natural lens is ignored as the lens is gone after the surgery. This does not meet the 0.75 minimum required for the lowest power toric, so my lens is not a toric version. I can fairly easily see the 20/20 line of the distance eye chart and about half the next line. Quite pleased with my distance vision overall even with the slightly higher than anticipated astigmatism.
.
As far as near vision goes it is much better than I expected. I can read a computer screen with normal font at about 18 inches, but it goes downhill rapidly at closer distances. I may be getting this vision to some degree because of the residual astigmatism which is minus. This said I don't think using a computer with both eyes corrected for distance would be that comfortable with a normal sized computer monitor. If one had a big screen further than 18" away it might be OK. But with my 24" monitor I like to sit closer. I see the instruments on my car and truck dash perfectly with the IOL eye. TV is great as well.
.
I am currently simulating monovision with a contact in my other eye. I got about 5 different brands and samples of different powers at Costco and settled on one that leaves me about -1.25 short sighted. Based on other lens powers I tried, I think -1.25 to -1.5 would be fine. I can sit more like 12" from the computer screen and I see fine. I can read my iPhone 8+ fine as well. Vision does eventually jam out when trying to read the super fine print on OTC medicine bottles and the like. That requires reading glasses.
.
I do have progressive lenses that fully correct both my IOL eye and my mild cataract eye for distance and near. For sure that is the crispest vision. However, I like the eyeglass free method with the monovision contact much better. I really only use the progressives when my one eye gets tired of the contact. But for the most part go eyeglass free about 16 hours a day.
.
I have thought about getting a Vivity in my second eye with -0.75 under correction to achieve monovision, but my current thinking is to go with the same monofocal lens again with -1.25 under correction.
.
I am not sure I would rush into the second eye in two weeks. There is no hurry. It takes 6 weeks of healing to know for sure what you get for vision in the first eye done. They normally target -0.25 for the distance eye, but it is not always achieved. You might get more or less. If it was really off to the minus side, you might want to switch which eye is corrected for distance.
.
If your vision is good enough I would suggest trying monovision with a contact lens to simulate it before you get the second eye done. Or if by chance you are left with -1.25 to -1.5 in the non operated eye, you could do it with no need for a contact.
.
Hope that helps some,
banterer Pifutoast
Edited
Hello,
I just had my surgery about 5 weeks ago and got the LAL (there is a thread here asking for people's experiences with it. I went into detail on my experience there and the results that I have obtained. I have had the first two adjustments (I hated the idea of monovision because I tried it with lasik and abhorred it! They then talked me into mini-mono and I hated it less.). However, monovision with these lenses is unbelievably natural (I'm R.E. dominant and was near sighted most of life up until lasik in 2004).
After this second adjustment, my right eye should be 20/20 and the left eye is supposedly 20/25 (though the left is mostly for close vision). Unlike most others on here, I am not familiar with all the opthalmic terms. I can only tell you that I can read and function without glasses now for all but something extremely tiny that would be very close up. Other than both eyes not being exactly the same, I do not think I have ever seen as well as I am right now.
If I were you, would do much more research and go in KNOWING as much as you could because with as much research as I did, I was still not fully briefed on what to expect. The beauty of this lens is that they can adjust it after your eyes heal so it can be tailored to yield the best results possible with the existing tech. There is a clinic (Codet) in Mexico that supposedly is doing EDOF adjustments with the LAL but I have not been able to find any documentation on their results. As far as my vision goes, I am EXTREMELY happy with it.
My recommendation is NOT to have surgery until you can make an informed choice/selection/decision you've made. Keep in mind that most multifocus lenses end up having visual artifacts at night due to having the sharp edges on the concentric circles to achieve the multifocality, so night driving can be a challenge (many concentric circles around light sources).
Hope that helps.
Guest Pifutoast
Posted
There are no absolute answers because the IOL is just one variable in a very complex system that can vary greatly from person to person. My Dad has Tecnis 9300 IOLs (monofocal) and can see clearly down to 1 foot. But surely that's extremely rare. Maybe he has extremely steep corneas or was overly undercorrected. Who knows. Others end up with results where everything within 5 feet is a blur. But on average I think the best you can probably count on with a standard monofocal is for your functional vision (maybe not sharp but functional) to start at around 3 feet. With Eyhance I think you can count on the 3 foot range being quite good and maybe a little bit of functional vision slightly closer. With Vivity I think you can count of pretty decent vision down to 2 feet.
.
As for Panoptix halos, halos are just physics. Everyone will get them. It's just the nature of the optics used. Everyone. BUT the degree of severity can vary from person to person as well as the ability of the person to just simply not look at them (i.e. ignore them / filter them out). But saying only a small percentage of people even GET THEM in the first place seems, from everything I've read, borderline deceptive. Today's diffractive lenses are apparently miles better than early refractive multifocals like the Rezoom which had horrible halos, and they improve with every new version, but they'll never get rid of them completely.
Pifutoast
Posted
Thanks for the replies so far. Another option, light adjustable lens???? There is facility near me that advertises this? Will look into it
I am postponing my surgery. More research needed, just not completely comfortable yet. I was at the consult/testing for 3 hours or more, saw the doctor for maybe 5 minutes and he seemed harried or in a rush. Advised on what he thought was best and handed me the marketing brochures. "any questions?? I had know idea what to even ask at the time and when I did have questions it was difficult to get anyone to answer, no number or extension except for the main reception. I feel they are too big to deal with the patients they churn out.
What do the numbers mean . 1.25 .75 etc, they never provided any information on where I'm at.
Pifutoast
Posted
Getting too complicated, argh...
RonAKA Pifutoast
Edited
You asked about the numbers. It would help if you could post what your current eyeglass prescription is for each eye. That will give some indication as to whether you will have temporary monovision until the second eye is done. Your prescription should look something like this.
rwbil Pifutoast
Posted
2)I think one of the reason doctors want you to get the other eye done right away, is sadly most people don’t do any research and binocular vision will be better and might solve their issue. I could write in detail on this issue, but can look at charts on binocular vision and see what I am talking about. My advice is wait long enough to see what your results are with the first IOL. Heck I had cataracts in both eyes and it has been 4 years and still waiting to do the other eye. See what the results from the first eye is and then make a decision. This would be one area that LAL would shine as you can adjust post op.
3)I would be more concerned about why my vision was poor from the first install and address that first.
4)Hmmm, I just assumed almost any Ophthalmologist would do monofocal monovision. I would find a doctor with lots of experience doing what you decide to do. Again this is why the LAL is revolutionary. You just don’t know what refractive mark the doctor will actual hit and what your vision will be like until after surgery. So I would want a doctor that has lots of experience doing monovision and takes the time to tell you about his patient’s results using various settings. Remember going to great on monovision can have adverse effects. Again until an actual adoptive IOL is approved there is no free lunch and it is about what tradeoffs you are willing to accept.
rwbil Pifutoast
Posted
First, good to hear from a fellow Floridian. Ron and Banterer have given you some really good advice and I think you are 100% asking the right questions.
A couple of things you said really hit home.
“More research needed, just not completely comfortable yet”
I am an engineer and researched all the information I could find before making a decision. No one cares about your eyes as much as you do, so do the research.
“I was at the consult/testing for 3 hours or more, saw the doctor for maybe 5 minutes and he seemed harried or in a rush.”
Been there!!!!! Not only did I do plenty of research, I went to several Ophthalmologists. One problem I had was I had done the research and in some cases knew more about the material and other issues regarding the lens then I think they did. One Ophthalmologists wanted to use the Restor IOL, I stated to ask about glistening and Abbie Number and you could visible see him getting unset that a patient dare to ask questions of this nature. I guess he thought this is a religion where you blindly follow his recommendation. I remember you find an Ophthalmologist that is top rated, been involved in clinical trials, an expert in the particular IOL you select and just as important one that you are comfortable with.
So don’t be concerned about shopping around. Not all Ophthalmologists are the same. I finally found a top rated Ophthalmologists in my area that was not rushed and would / could intelligently discuss the issues I was concerned about.
Also if you are in Southern Florida I talked with Toby Tyson and he spent time talking to me about the entire history of various IOLs and his experience with them. But he was a bit of a drive for me and I finally found an Ophthalmologist near me that I liked.
As for halos, I have a MF IOL in one eye and IMHO everyone who gets a defractive lens gets halos. Heck you can get them with a monofocal IOL. It is a matter of how much they bother you. I read someone else explanation of what really happens and it was so much better than how I would have explained it I will paste their words and it also applies to defractive EDOF IOLs:
“To be clear, multifocal visual disturbances never "go away". You can't change physics. A more accurate thing to say is that the brain habituates to them. The visual disturbances are still there and if you THINK about it you will see then exactly the same as you always have. It's just that if your DON'T think about it you don't notice it. You brain learns to "filter them out". But they're still there.”
There is no perfect lens selection for everyone. You need to take your time and think about what activities are most important to you. Only you can decide what tradeoffs you are willing to accept. If your 100% sure you want to reduce the risk of halos, starburst and other dysphotopsias, below is my list of refractive IOL option in order of risk:
Non Premium Monofocals:
These are the most common Iols implanted. They will have the best contrast and the least issues of any lens (unless you consider close vision an issue). They have been around and tested for a long time. A Monofocal lens should provide great distance. In general close vision is reading your cell phone or a book, maybe 33cm-40cm. Intermediate is about 2 feet or so. A perfect example might be the dashboard on your car.
One comment on distance vision. Some people I think are confused by that term. If you look at the defocus curve on a monofocal you should get pretty good vision down to about 2 or so’. As you get in closer; vision quality drops off rapidly. This is important, everyone Visual Acuity will vary as there are so many factors, such as short eyes, astigmatism, previous Lasik surgery, and on and on.
I also suggest just getting 1 eye done at a time and evaluating the results before getting the other eye done. Mix and Match is always a possibility to obtain the best vision possible.
Premium Monofocals:
LAL – If considering a monofocal I would recommend giving this IOL serious consideration. I have had Top Ophthalmologist highly recommend this lens. Having said that it has been around for a while now, but not as long as the standard monofocal so there is the test of time issue.
What makes this lens great is no matter what equipment Ophthalmologist use they don’t always hit the refractive mark and in a few cases can be way off by more than 1D. And let’s say you decide to do monovision. You want to hit those marks.
But it even gets cooler than that. From what I understand you can adjust the LAL more than once. So you decide on monovision, but not 100% sure how much monovison. So set 1 eye to plano and then try various settings with the 2nd eye to see which one works best for you. I would only consider micro-monovision like -0.75D, but if I had the option to adjust it you could try a different setting and see if you end up with a lack of stereopsis or other problems.
Crystalens Lens – You hardly hear about this lens anymore. This is the only FDA approved accommodating IOL. Many people did not get accommodation or much accommodation, so you were paying premium price for a monofocal lens that did not give the range of vision expected.
But from what I have read Crystalens at distance provides the same level of contrast as a standard monofocal and you are likely to get some accommodation. This lens could be a great mix and max with a PanOptic Trifocal IOL.
IQ Vivity and Tecnis Enhance - The newest hottest IOLs on the block. A refractive IOL that provides some EDOF. I think IQ Vivity is around .5D and Eyhance a little less. So not a lot but combined with micro-monovision you should get decent intermediate and some close up vision.
Now here is the part that is trick. I have read that Vivity gets EDOF by manipulating SA. So that means contrast sensitivity will not be as good as a standard monofocal. Could the average person notice the difference, I don’t know. But I suggest you get an Ophthalmologist who is an expert with these lenses so you can discuss that exact issue. And of course there is the test of time issue.
I tried mono-vision with contacts and I know it is not the same, but I hated it. I need good distance vision. That is why I say if doing mono-vison go with micro-monovision (<-0.75D). If you do that with Vivity you will be getting -1.25D of mono-vision, preferable in the non-dominate eye.
I have the Tecnis Low Add MF +2.75 in my left eye and my natural lens in my right eye. This means I get dysphotopsias. But the trade-off is worth it to me. I get Functional Close. What that means is I can see a menu in a restaurant or read a label at a grocery store. And yea if I find the right sweet spot I can read an article, but to do any serious reading I need a good light and readers.
In full disclosure I am currently thinking about implanting the Synergy IOL into my right eye, once it becomes FDA approved and there has been more published reports on Real-World results. The Synergy, hands-down, has the best defocus curve I have seen , which already makes me worry about how “bad” the trade-offs will be.
Keep me posted and if you ever head up to Northern Florida give me a shoutout.
Pifutoast
Posted
Thanks for the replies, really helpful. I uploaded the eye exam results, but it's from last August, most recent I can't find. Maybe the optometrist didn't give me one, since he sent me for a cataract consult? Any comments on what it shows?
I might actually get it done tomorrow, mono focus set to distance with taking a wait and see approach. I am used to wearing glasses for reading anyway, if that's the worst of it I don't have a problem with that.
Probably the safest, certainly less expensive way to go. As I've been learning, it's going to be a compromise no matter what.
My feeling about St Lukes Cataract and Laser institute. I feel they are good at the install, as they have state of the art equipment and very experienced docs, however, not good on a personal level to work with you to have a plan to implement the best strategy for success. I suspect most people simply go with whatever is recommended to them and don't question anything. They are certainly not set up for it. More of factory approach. First eye, 1 week follow up, second eye a week later, keep the conveyor belt moving.......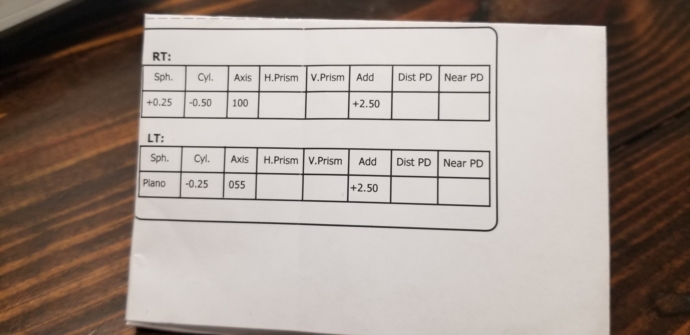
Pifutoast
Posted
One more thing, do I need to find out what mono focal lens they use? Are there any to avoid that I would postpone the procedure over,
thanks again
Pifutoast
Posted
Had surgery as scheduled after struggling with which lens to go with. I opted for mono focus for distance.
Too early to tell where I'm at, but the sharpness and clarity and color are incredible. My uncorrected left non dominate eye is 20/150 . I didn't realize how bad my cataracts were until now. shifting between eyes like switching from warm yellow to daylight
I can read from about 12-18 inches without glasses with both eyes open. 3 days out. looking up is a little disorienting.
The installed mono focal is a B&L model A060, power 18.5D.