Symfony already implanted (dominant eye), I chose to implant Synergy in the other eye.
Posted , 7 users are following.
For those who followed my previous post "Symfony already implanted (dominant eye). Which one to choose for the other eye, Synergy or PanOptix?" and wait for an update. And also for those who might be interested in my experience...
Since 12/06/2021 I have a Symfony lens implanted in my left eye (dominant) and yesterday, 03/30/2022, a Synergy lens was implanted in my right eye (non-dominant). Both lenses were calculated for emmetropia. I got a good result with Symfony, and I hope to get a good result with Synergy too. As today is only the second day after the surgery, I will keep updating when something new happens...
Regarding the surgery, everything happened in the same way as in the first one, when Symfony was implanted. I was prepared in surgical clothes, taken to an operating room where my eye doctor, an anesthesiologist and a nurse were. I had the chance to say hello to my doctor, he asked me to lie down on the surgical bed and I did, he asked if I was comfortable and I said yes, so the anesthetist introduced himself and explained to me, in detail, everything he would do (I remember very little of what he said) and stuck a needle in my arm, then my doctor asked me to open my eye and dripped a drop saying it was the anesthetic, moments later (at least for me...), he said everything went well well in the surgery and that I could get up. The advantage of deep sedation is that I don't remember anything about the surgery itself, and the disadvantage is that I don't have much to tell.
Right after the surgery, my vision of the operated eye was very blurry, cloudy and very dark. As far as I can remember my first surgery (Symfony), I feel that my vision is a little better than it was at the first moment with Symfony, except for the dark vision which, even in a well-lit environment, seems to have half the brightness it should have. . This worried me a lot!. To give you an idea, last night in my room, with all the lights off, my Symfony eye can still see the shapes of the bed, chair, closets, the lights in the cracks in the doors and windows, in addition to the LED's indicators of electronic equipment. , etc. But closing the Symfony eye, and trying to see only with the Synergy eye, it's TOTAL DARKNESS! It's like I DON'T have my right eye anymore! A terrifying sensation!
Today, when I woke up, I noticed that it improved a little, less blurring and less turbidity, however, floaters appeared, the interesting thing is that yesterday I didn't see them, maybe they became visible due to the little improvement. But that didn't worry me, since it had also happened in the first surgery (Symfony), and after some time, they "disappeared" (or I stopped seeing them). As for dark vision, it continued to worry me. I returned to the hospital for the post-op consultation and saw my ophthalmologist. He examined me in the slit lamp and said everything is fine, the lens is well centered, but the cornea is still swollen. When I asked about the dark vision and my concern about it, he smiled for a while and said that I didn't need to worry, because it was the effect of a myoptic eye drops that he applied to my eye at the end of the surgery, exactly to promote the contraction of the pupil, and that it will be contracted for a few days, so in low light I wouldn't see well at all. He even asked me for feedback on how long this effect will last in my case. I asked if he had used these drops when he implanted Symfony and he said yes, but I'm not really sure about that. I didn't know what to think!? At the same time that I felt some relief, I was in doubt if it is normal to use this myoptic eye drops after cataract surgery, because in my first surgery I did not have this effect, in fact it was the opposite, I even had to wear sunglasses , how bright was my vision?!
I have not had the luck of some, who can see very well the day after the surgery (in none of my eyes), but I continue with the eye drops hoping to get the desired result.
Any significant changes I update.
Thanks.
0 likes, 46 replies
soks valerio01538
Posted
thanks for the update.
valerio01538
Edited
Today marks 2 weeks since the surgery. I still have little improvement. Slightly blurred vision as soon as I wake up, at any distance, which will only get better as the day goes on. Tried using eye lube (thanks @rwbil) but didn't feel any difference. Even when vision improves, Symfony's eye still has much sharper vision at a distance. In these last 3 days, it started to flicker at various times of the day, even with the normal light of my work room. I had this with Symfony, but it was only for the first week and a few moments, and only in sunlight. Another thing I've noticed, is that I'm having some difficulty choosing the best distance between 12" and 20", it seems my brain prefers my Symfony dominant eye and doesn't want to allow my Synergy eye to take over. After working a few hours on the notebook, Symfony's eye starts to burn and hurt a little. I have a question that I've done some research, but haven't found the answer: The more the corneal edema, caused by the surgery, is cured, the tendency is for the vision to go more myopic, hyperopic or is there no such change? I continue with the drops...
rwbil valerio01538
Posted
I can only tell you for me it took longer for my Synergy eye's vision to get sharp, compared to the time it took for my MF eye. My MF was sharp the next day.
Today, many months later I did the one eye at a time thing and I see better distance with my MF and better close with my Synergy. But it is not a big difference for distance, just a little better with my MF. I don't know if this is due to the Synergy IOL itself or residue refractive and /or astigmatism in that eye.
You do make an interest point with brain adaptation and different people could see different results.
Give it at least a month for eyes to heal and brain adaptation to kick in.
RonAKA rwbil
Posted
If you get a simple eyeglass refraction test you should be able to tell where you ended up for sphere and cylinder in each eye. My surgeon only does the quick and dirty autorefraction after surgery (look at the red barn or hot air balloon image on the horizon). He said my last eye was at -1.25 D sphere, and right on target. When I went to my optometrist he did the full refraction test and measured -1.0 D sphere and -0.75 D cylinder at 67 deg. Prior to surgery I was -1.25 D and -1.25 D cylinder at 077 deg. I think that is the first step in understanding what your vision is doing -- at least for distance....
rwbil RonAKA
Posted
They did the standard look in the eyeglass machine, where they flip between 2 lens and ask is 1 or 2 better. Not sure what the official name for that is.
Doctor said no correction needed. But there are so many factors like maybe the astigmatism is not all regular in that eye. Who knows.
And bilaterally I don't notice it. I only notice it if I do the cover one eye up at a time thing. And it is not like a huge difference, but everyone is different.
valerio01538 RonAKA
Posted
After reading their recommendations on more than one occasion, I managed to see an optometrist 1 week before my second eye surgery, just out of curiosity to know where the sphere and cylinder of my first (operated 4 months ago) ended up. She took all the measurements, but didn't want to give me the results, she just told me that she wouldn't need to prescribe any corrections in my case. But during testing, I noticed that it stayed longer on charts that test for astigmatism, so I think I must have some. Now I realize that I shouldn't have explained in detail to her that my intention was to verify the outcome of the surgery. I believe she didn't want to give me any information that would cause any conflict with my eye doctor. She ended up not even charging for the consultation, but she assured me that everything was fine. I will try to contain myself and wait for both eyes to heal and stabilize well before going back for any checks.
RonAKA valerio01538
Posted
Yes, it seems to be part of the eye care politics. I always ask for a written eyeglass prescription from the phoropter ( which is best, one or two) measurements. When one does the 3 week post surgery they will give you a verbal report, but will not write a prescription based on my experience. At 6 weeks they should give a prescription. They don't want to get caught being blamed for a bad prescription because it was written too soon after surgery. Regardless of whether or not I am going to get glasses I ask for it so I have an accurate measure of where my eyes were at at that point in time.
.
Part of the game is that, at least here, there will be an optical supply store at the same site that the optometrist does the exam. Often the optometrist is an owner or part owner of the shop, but legally it has to be a separate company. And, they want you to buy your glasses there, as that is where the real profit is. They don't make much on an eye exam, but in private shops the markup on eyeglass lenses and frames is astounding. For that reason they don't really want to give you a written prescription that you can take to shop around for the best price on glasses, or to buy from on line places like Zenni.
.
For us it is the best check on how well the outcome was from the cataract surgery. Was the right power used for sphere? Was the right power used for astigmatism? Is the toric lens at the right angle to provide correction?
valerio01538
Posted
Yesterday (20/04/2022) I went for my 3 week follow-up appointment. They took measurements on the auto-refractor (red balloon) and then referred me to my ophthalmologist's room. He examined the placement of the lens with the slit lamp, said it is in the correct and centered position. He did distance and near vision tests (binocularly). I was able to see 20/15 and J1+. I asked about the results of the auto refractor. He said the device makes 4 concucutive measurements. Symfony measured cylinder: -0.25D/0.0D/0.0D/+0.25D which, according to him, this sometimes happens, but he considered the average 0.0D. Synergy measured cylinder: 0.0D on all 4 measurements. Also did tests on the manual refractor (1 or 2, which is better?) and the results were the same as the auto refractor. I asked him to explain to me if everything is ok, what is the reason I have a little blurred vision in Synergy. His theory is that EDOF lenses take much longer to neuroadapt than other lenses. With multiple images hitting the retina due to the echelette design of the lens, it ends up stimulating new areas of the retina that were not stimulated before, and the brain needs more time to deal with it all. He believes that after a while, the brain will filter, choosing only the image that is more focused, improving quality. He recommended that I try not to use any correction lenses (either near or far) to "force" this neuroadaptation for better vision without glasses. He scheduled my return only for 6 months from now. So, I hope this neuro-adaptation really happens...
RonAKA valerio01538
Posted
For sure a MF lens is going to present the eye with different images that are not all in focus. It makes a lot of sense that it will take some time for the brain to sort out which one to choose as the right one. If you are testing well, and it seems you are, then it makes sense to give your brain some time to adapt.
Sue.An2 valerio01538
Posted
Hope things improved. Was away for awhile and just catching up.
I had 2 Symfony lenses implanted in 2017 and could see quite well after first surgery and 2nd one took a day longer. Sometimes there is more swelling or eye drops affect it more - I wouldn't worry in the early weeks.
valerio01538 Sue.An2
Posted
Yes, things seem to be getting better every day, thank you! Every day I feel like my eyesight is improving compared to my Symfony left eye which is still a little better from a distance. The Synergy eye looks like it is now being able to "impose itself more", giving me better up-close vision. I still have a week with the eye drops (ketorolac trometamol), I don't know if it interferes much with the quality of vision...
Sue.An2 valerio01538
Posted
Glad to hear things are improving. For many people the drops do make vision blurry for a bit then clears till next round of drops.
valerio01538
Posted
These last 2 weeks has been a bit busy! My general vision is good, but the distance vision of the Synergy eye is still not as good compared to the Symfony eye. My near vision has stabilized and I can use the phone at 13", but to see the details of HD photos and videos well, I need to move the phone away to 16", honestly I expected a better result than this. Dissatisfied and, with the intention of trying to understand this result, I decided to ask the Hospital where I had my surgeries to send me all the results of my preoperative exams and, to my surprise, I received it in my email (I didn't know I could have access to them, otherwise I would have request before!). Attachments to the email came: Corneal Topography, Retinography, Specular Corneal Microscopy and 2 Ocular Biometries, one made for the Symfony eye and the other for the Synergy eye. Now I know that the Optical Biometer used was the AL-SCAN NIDECK. I did some research and it doesn't have the same accuracy as an IOLMaster 700, but it's not the worst either. In biometrics, I found that, in addition to all the measurements needed to calculate the power of the lenses, there is already a pre-calculation for a dozen lenses, using the formula HOLLADAY1. The results of the calculations are presented in 7 powers to be chosen, each one with its possible predicted residual refractive error. The central result is highlighted and has the smallest predicted residual refractive error. There are still 3 more results pointing to hyperopia and another 3 pointing to myopia, with their respective predicted residual refractive errors. As I understand it, if the ophthalmologist is targeting emmetropia, he should choose the centrally highlighted result with the smallest predicted redidual refractive error. Following that reasoning, I verified that the highlighted power for my Symfony eye was 20.0D with a predicted residual refractive error of +0.08D, which was exactly the power shown on the Symfony lens card. The highlighted power for the Synergy eye was 19, 5D with a predicted residual refractive error of -0.04D. That's when my worries started, because the power my ophthalmologist chose (which is on the lens card) was 19.0D, that is, 0.5D less. As he had told me that he uses the Barrett Universal II formula for the calculations, I now have my biometrics, I did the calculations myself using the BU-II formula and the result was exactly the same as 19.5D. I honestly don't know why he chose a power 0.5D less (I'll have to ask him...). I made an appointment with another ophthalmologist at another clinic for verification. The results I got confirmed my suspicions and surprised me too! From a distance my vision on Symfony is 20/20, and it's 20/25-2 on Synergy. In tests with Phoropter, she came up with results that indicate a prescription for distance glasses of +0.5D sphere for both eyes and -1.0D cylinder for the Symfony eye only (I didn't expect this). For close-up, I need a +1.0D addition to both eyes. I wonder how much better my vision would be if there weren't these refractive errors. In view of these results, I will be scheduling a return visit with my surgeon, waiting for him to explain this situation to me, because at the last appointment he said that everything was 0.0D...
valerio01538
Edited
Biometrics attachment. It has inscriptions that are in Portuguese: "Direito"=eye right, "Esquerdo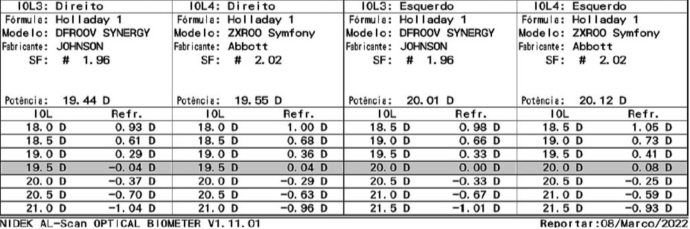 "=eye left.
"=eye left.
RonAKA valerio01538
Posted
It looks to me that the surgeon did not target the usual -0.25 D myopia or a little more, and should have used the next higher power lens in both eyes. You really do not want to end up with a +correction for distance.
RonAKA valerio01538
Posted
I don't think the Holladay is the best formula, but given those choices I would have picked the 20.0 D in the right, and 20.5 D in the left.
.
These are the kind of screen shots that the patient and surgeon need to look at and discuss before going ahead with the surgery. I have seen a similar screen from a write up on the Zeiss IOLMaster 700. It is capable of doing a grid display of multiple formulas at the same time so you can look at how the formulas differ and what your options are for power in each one
valerio01538 RonAKA
Edited
Do you understand now why I'm interested in LASIK too?! I have been following your posts, reading the articles you have indicated and I feel that there is no way to correct this error of +0.5D. And the other ophthalmologist told me that the -1.0D cylinder error in the Symfony eye, is even helping me see better up close, compensating for the +0.5D sphere error.
RonAKA valerio01538
Posted
I would have to agree, that like me Lasik does not look like a good option when trying to correct small amounts of hyperopia. What I am starting to understand is that the predictability seems to be a fixed amount, not a relative amount. So when correcting +5.0 you may hit within +/- 0.5 D of that if you get really good results. And the patient is likely to be very happy if they get somewhere between -0.5 D and +0.5 D, compared to being +5.0. But when correcting +0.5 D then the error may still be +/- 0.5 D. So you could end up anywhere from 0.0 D (happy) to +1.0 D (twice as bad!).
.
I have not totally eliminated this option yet, and I am waiting to hear from the surgeon that is probably the best and has the best equipment in our city. If he says no it can't be done, then that will be the end of the road. And, in fact I am getting so nervous about making things worse, that I may decline in any case unless he gives me lots of confidence he can make it better, not worse!
.
All of this is suggesting that if the plan is to use Lasik to do a post surgery touch up then you want to end up on the myopic side of optimum, as it is easier to correct with Lasik. Correcting myopia requires laser incisions close to the center of the eye, while correcting hyperopia requires incisions out at the periphery which are less predictable.
valerio01538 RonAKA
Edited
"I don't think the Holladay is the best formula, but given those choices I would have picked the 20.0 D in the right, and 20.5 D in the left."
I also calculated by BARRETT UNIVERSAL II and the difference was negligible. From what I've researched, HOLLADAY1 is pretty accurate for average eyes.
RonAKA valerio01538
Posted
The one study I found showed there were more differences between the formulas when targeting myopia for monovision than for targeting emmetropia. Here is how the formulas ranked for accuracy based on being within +/- of 0.5 D in the emmetropia distance eye:
.
Barrett Universal II - 87.5%
Hill RBF 2.0 - 86.4%
Haigis - 85.2%
SRK/T - 83.0%
Holladay I - 78.4%
Hoffer Q - 75%
.
This study did not distinguish based on eye axial length, but your eyes must be pretty average with a 20 power lens need.
.
OPTIMIZING OUTCOMES WHEN THE TARGET IS LOW MYOPIA ANDREW M.J. TURNBULL, BM, PGDIPCRS, FRCOPHTH; WARREN E. HILL, MD; AND GRAHAM D. BARRETT, MB BCH SAF, FRACO, FRACS PDF
Myope_PSC valerio01538
Posted
Google "tecnis_synergy_iol_getting_started_guide_updated" and download the PDF file for interesting info about the Synergy lens and the explanation for when to target the first plus. The instructions to choose first plus is when first plus and first minus are equal for the Synergy lens according to the guide.
Your right eye's first plus and first minus are close to equal but not actually equal. Coincidentally, your left eye's first plus and first minus are equal.
valerio01538 Myope_PSC
Posted
Your observation is very interesting, thank you! I had downloaded this J&J Synergy Lens guide some time ago, but I didn't remember this information on page 9, which shows this example case. It says that only when there is exactly the same error, one for plus and one for minus, should you choose the first value of power plus, while in other cases, you should always choose the power with the error closest to zero. In my case, if you observe, all 7 powers are valid (from 0.5D to 0.5D), so the closest error to zero is even -0.04D, which corresponds to a power of 19.5D , confirming that this would be the best choice.
RonAKA Myope_PSC
Posted
The J&J guidance seems to ignore the impact on closer vision. Yes the drop off slope is less on the + side, than on the - side. But the drop off slope in the near vision is steeper still. The issue with going hyperopic is that it costs both distance and close vision. Going myopic hurts distance, but helps close vision.
valerio01538
Edited
Sorry for the technical content, but it might interest some. I read this article: "SCIE-04557-RESEARCH_ARTICLE-KANAR.pdf" which compares the AL-SCAN biometer with the IOLMaster 500 and found that AL-SCAN determines corneal power (K1, K2, KM) a little differently than Master IOL. Without going into too much detail, AL-SCAN takes two measurements, one on a 2.4mm diameter and one on a 3.3mm diameter. In the article, it was verified that the measurements made in the diameter of 2.4 mm, presented more accurate and comparable results to those of the IOLMaster. That said, I recalculated on the BARRETT UNIVERSAL II formula using the K1 and K2 values for 2.4mm, and found different values for my lens power compared to the values calculated by the HOLLADAY 1 formula from my biometrics. Maybe that explains my surgeon's choice, but it doesn't explain the outcome.
RonAKA valerio01538
Posted
It is interesting that there is a difference. Was this with the same Symfony and Synergy lens choice? In any case with this data I think the easy choice with the right eye would be the +19.5 D. The harder choice would be the left eye. The +20 D would be risky and the +20.5 the safer choice.
.
My surgeon has done one of my wife's eyes and both of mine. In all three the outcome has been 1/4 to 3/8 D more hyperopic than what he said was the expected outcome. Fortunately for emmetropia he targets about -0.25 D. My wife's outcome was 0.00 D, and in my distance eye the same at 0.00 D. Unfortunately in my close eye the 0.25 shift to more hyperopic was not as good for me. I think he used Hill RBF II on all of them, but not absolutely certain.
.
His comments on targeting emmetropia is that he always likes to be a bit negative because nobody ever thanks him for going positive....
valerio01538 RonAKA
Posted
These calculations I made for 2 Synergy lenses, but the constant A (provided by J&J) of the two is the same (119.3), only the Lens Factor (SF) changes, which in Synergy is 1.96 and in Synfony is 2.02, but it changes a lot little in the result. I've noticed that my surgeon is always aiming for emmetropia and leaving his patients a little hypermetropes, I'll talk to him about it.