Nocturia getting worse - does this sound familiar? Any ideas appreciated!
Posted , 13 users are following.
I am 72 years old, and other than the prostate issues, am in excellent health. Work out 3x per week, not overweight, no sugar or junk food.
Had successful treatment for prostate cancer (radiation) in 2014, and a PAE for BPH issues in 2017. The PAE was only partially successful due to median lobe issues.
Now, I am up to two Tamsulosin per day, and my trips to the bathroom are increasing. At night I am up every hour to hour and a half and it takes me 10-20 min each time to clear enough urine from my bladder so that I can get back to sleep. My latest measured PVR was 200ml.
Here's what happens at night: my bladder wakes me up with the message - you have to pee. I go to the bathroom and pee out about 50-75ml. Then, I try to go back to bed, but I still have that sensation in my bladder that I have to pee - so can't get back to sleep. Then, it's back to the bathroom again. I am now up to 3-5 of these repeat peeing attempts before I can actually get to sleep. This condition is getting worse.
I have been able to get some relief by taking Trospium (for overactive bladder), a small amount of melatonin, and Tylenol before going to bed. The Tylenol seems to dull down the bladder irritation.
I have had many urine culture tests and I do NOT have an infection.
The lack of sleep is wearing on me. I have to do something, and I know this decision is coming up soon. My only three options (based on my insurance, location and finances) is a second PAE, a bipolar TURP and Greenlight. Urolift won't work for me because of the median lobe.
I hate to take my little fistful of pills before bed (the second Tamsulosin, Trospium, Tylenol and melatonin), and recently added a few drops of Passion Flower liquid. Anything to help me sleep.
Does any of this sound familiar? Any ideas that might help me would be appreciated.
Tom
0 likes, 40 replies
stan98754 tom86211
Posted
Hi Tom,
I have had very similar symptoms like you . Nocturia, lack of sleep, PVR 200-250 ml and same reason - big median lobe acting like pressure ball valve . Buying time with CIC for 2 years ,but serious bladder damage,sphincter damage , and some urethra stricture occured. I started investigation how to avoid drastic TURP and similar operation and found PAE . But NO effect after it in Lisbon Portugal in May 2017 just due to median lobe IPP ( intravesical protrusion of prostate ). So you need exact diagnosis
firstly. This is possible ONLY by well made MRI 3 T scan . Ultrasound image is not sufficient. My MRI scan showed IPP of grade III as you can see in image. You can find about IPP many articles , for instance ...
IPP of grade III as you can see in image. You can find about IPP many articles , for instance ...
Intravesical protrusion of the prostate as a predictive method of bladder outlet obstruction.
Reis LO1, Barreiro GC, Baracat J, Prudente A, D'Ancona CA.
Abstract
OBJECTIVE:
Pressure-flow study is the gold standard for diagnosis of bladder outlet obstruction (BOO). A prospective study was carried out to compare urodynamic evaluation and measurement of intravesical protrusion of the prostate for diagnosing BOO.
MATERIALS AND METHODS:
Patients presenting with lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia and suspected BOO were prospectively evaluated through conventional urodynamics and classified according to the bladder outlet obstruction index (BOOI). They also underwent abdominal ultrasound measurement of the intravesical prostatic protrusion (IPP) and prostatic volume. The IPP was classified into three stages: grade I under 5 mm; grade II, between 5 and 10 mm; and grade III over 10 mm.
RESULTS:
Forty-two patients, mean age 64.8 +/- 8.5 years were enrolled. Transabdominal ultrasound determined a mean prostatic volume of 45 +/- 3.2 mL. Achieved IPP's values were the following: grade I - 12 (28.5%), grade II - 5 - (12%) and grade III - 25 (59.5%). The results of prostate volume differed significantly between obstructed and non-obstructed men (p = 0.033) and for IPP among obstructed, inconclusive and non-obstructed men (p = 0.016). For IPP, the area under ROC curve was 0.758 (95% confidence interval - 0.601 to 0.876), and the cutoff point to indicate BOO was 5 mm with 95 % sensitivity (75.1 - 99.2) and 50 % specificity (28.2 - 71.8).
CONCLUSION:
IPP and prostatic volume measured through abdominal ultrasound are noninvasive and accessible methods that significantly correlate to urinary BOO, and are useful in the diagnosis of male urinary obstructive problems.
.......................
Due to some stricture of urethra was not possible to use any transurethral method - invasive ( TURP, Green light, etc... , or miniinvasive ( Urolift, REZUM ) .My problem was so bad in the beg. of 2018 - 300-350 ml PVR, no sleep, infection, CIC every 8 hours,bladder damage, incontinence ,... so urgent solution was needed. After many months of investigations, consultation I found proper alternative just for my problem -FLA. Consulted by email and phone many times with Dr. K in Houston I finally decided for this method. Flying at route Vienna- Istanbul - Houston ( Im from Central Europe ) underwent at April 4th 2018 FLA procedure with Dr. K team. Now I'm nearly 1 year after and I can name it as return to life. No PVR, No CIC, No medication, no ED and NO RE ( retrograde ejaculation ) so my sexual life returned 10 years in time machine ( Im 65 ) . Then I even start to collect FLA patients with many criteria to Excell table and from about 30 patient I have just 2 failed and 2 mixed results. What is reason of fail in those patients according to analysis of data ?
I strongly reccomend you to made MRI 3T scan and then consult it with Dr. K in Houston. He is extraordinary man . Good Luck Tom. ......... Ave, Caesar , morituri te salutant ..... Stan
rdemyan stan98754
Posted
Stan:
I've been considering a 3T MRI for some time now. On the picture, am I correct in assuming that the arrow is pointing to a large median lobe protruding into space normally occupied by the bladder? Thanks.
tom86211 stan98754
Posted
Stan,
I really appreciate your reply. I have already been in contact with Dr. K in Houston. Unfortunately, I can't afford the out of pocket cost and due to work and family obligations can't take the time to go to Houston, so I will have to deal with this here. The sleep issue is getting worse - up, down, up, down etc. Wearing me out.
Tom
stan98754 tom86211
Posted
Yes Tom & Rdemyan ,
you see in picture extremally big IPP protruding to bladder , normal anatomy is smooth shape near bladder neck. In my case this BEAST IPP is fully blocking bladder neck and acting like ball pressure valve. As bigger is hydraulic pressure from urine in bladder as bigger is blocking of bladder neck by IPP . Even CIC was problematic in my case and many time I damaged ( bleeding ) bladder neck and IPP in final part . So my life was real hell in last months.
I know FLA is expensive ( 21K) , but its price of average car ( which will rost in 5 years ), but in my case saved my life. Yes I have had here in Central Europe another cheaper option covered by insurance - TURP, even REZUM ( in Germany ) , or green light., but all these method are transurethral . In my case due to many injuries of urethra ( CIC, infection ) there was developed some Urethra stricture, so transurethral tratment was unpossible. it could cause serious damage of uretra and in addition in case of such big median lobe the result is fully uncertain and could lead to serious bladder neck damage with next incontinence, ED, RE ,e.t.c.
Thats why FLA ( focal laser ablation ) provided via anus was only option. This procedure tooks 4 hours , where Dr. K milimeter by milimeter under full control of MRI boiled excess tissue in median lobe, and near urethra . After procedure I was able to return to hotel by my own and next day even walk in near park . Of course I have 1 week Foley catheter .
So as first step you need well made MRI scan to have clear picture about anatomy of prostate . and just then after consultation with more then 1 uro doctor and 1 IR ( interventional radiologist ) doctor decide about next step. Enclosed you can see anatomy during FLA operation.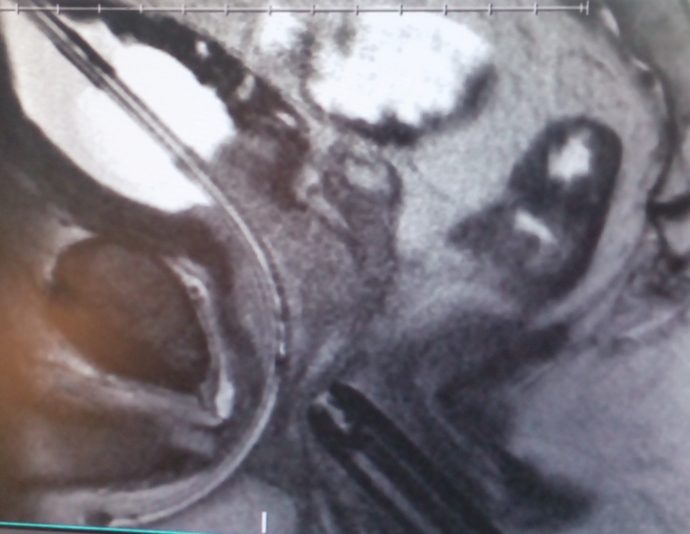 . Happy decision my friends and sorry for my english 😃 , Stan
. Happy decision my friends and sorry for my english 😃 , Stan
dcooperxyz tom86211
Posted
Learn to CiC, After the first couple of times its very very easy. Lots of information about it on this forum. This will ensure your bladder is empty. .Id go for that rather than surgery pesonally.
good luck
tom86211 dcooperxyz
Posted
I did do CIC a few times and it was very difficult for me - basically am afraid to try again. The reason I am leaning toward the surgery is that I just want this issue solved once and for all. The lack of sleep is becoming a crisis.
Tom
barney34567 tom86211
Posted
Have you had your hormones checked? If you, like me, have very low testosterone, then that will disturb your sleep and aggravate nocturia.
Do you drink anything 3 hrs before bedtime? If so, please stop.
tom86211 barney34567
Posted
Barney,
I have not had my hormones checked - never thought about that. I do drink soymilk, so perhaps that is doing something - what do you think?
Tom
barney34567 tom86211
Posted
Stop the soy milk pronto.
I have only read negative things about it.
It is full of estrogen and when you're a PCa patient
in time your testosterone level falls.
Adding MORE estrogen only increases the gulf between your
estrogen and testosterone levels.
tom86211 barney34567
Posted
Barney,
I make a couple of high protein blender drinks every day, and get the unsweetened soymilk. High protein, very low sugar content. Trying to stay off sugar as much as possible. My fasting glucose tends to be a bit above normal, so I read the nutrition labels and try to keep any sugars to a minimum.
Are you thinking that the soymilk may be causing some prostate enlargement?
Tom
rdemyan tom86211
Posted
If you want to get off soy, you can use other vegetable proteins such as pea protein or pumpkin protein or combinations. I like pumpkin protein.
Howard31850 barney34567
Posted
Is Almond milk ok?
barney34567 tom86211
Posted
Soy is plant based estrogen. When one has treatment for PCa one's testosterone is clobbered and the ration of testosterone to estrogen changes greatly. Consuming soy only makes the ratio worse.
The changed ratio causes disruption to a man's hormonal balance.
steven05114 tom86211
Posted
If your nocturia getting worse and you have already had one procedure to clear the obstruction, then the obstruction is back so your options at this time are to either have another procedure again to clear the obstruction that has returned or to start self-cathing. You can choose the procedure.
.
If you self-cath before bed, then that should get you through most of the night. I had a Rezum a little over 3 months ago which was successful in clearing the obstruction but due to bladder damage, I self-cath before I go to bed to completely empty. The result is that I get up only once overnight.
tom86211 steven05114
Posted
Steven,
Tried to self cath a couple of weeks ago - terrible pain, complete failure. Not going to go through that again. I am scheduled for a bipolar TURP next week. Have no choice. Sleep is completely disrupted by inability to clear my bladder. I wish I could do the self cath. My urethral lining is very sensitive.
Tom