Hypothermia
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Philippa Vincent, MRCGPLast updated 23 Dec 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
What is hypothermia?
Hypothermia is defined as a core body temperature below 35°C. Hypothermia belongs to the lethal triad (with coagulopathy and acidosis) for trauma victims requiring critical care.
The drop in core temperature can be rapid (as occurs in immersion in near-freezing water) or slow (as in prolonged exposure to more temperate environments). The effects of hypothermia are proportional to the change in temperature, with metabolic rate reduced in proportion to the fall in core body temperature.
Classification
Hypothermia is usually caused by accidental exposure but may be caused or aggravated by underlying medical conditions or may be deliberate as part of patient therapy.
Primary hypothermia
This is due to environmental exposure, with no underlying medical condition causing disruption of temperature regulation:
Trauma patients are particularly susceptible to hypothermia.
Perioperative hypothermia:
Hypothermia may be deliberate (see below) or accidental.
Any patient whose core temperature drops accidentally below 36°C at any stage of the perioperative pathway (from the hour before induction of anaesthesia until 24 hours after entry into the recovery area) should be warmed using a forced air warming device.1
Secondary hypothermia
This is low body temperature resulting from a medical illness lowering the temperature set-point:
Decreased heat production - eg, hypopituitarism, hypoadrenalism, hypothyroidism, severe malnutrition, hypoglycaemia2and neuromuscular disorders.
Increased heat loss - eg, vasodilatation (pharmacologic or toxicologic causes), erythrodermas, burns, psoriasis; or iatrogenic - eg, cold infusions, over-enthusiastic treatment of heatstroke or emergency deliveries.
Impaired thermoregulation - eg, trauma affecting the central nervous system, strokes, toxicologic and metabolic derangements, intracranial bleeding, Parkinson's disease, brain tumours, Wernicke's disease, multiple sclerosis, sepsis, multiple trauma, pancreatitis, prolonged cardiac arrest, and uraemia.
Drug administration; such medications include beta-blockers, clonidine, meperidine, neuroleptics and general anaesthetic agents.
Ethanol, phenothiazines, and sedative-hypnotics also reduce the body's ability to respond to low ambient temperatures.
Therapeutic hypothermia
Hypothermia with intracorporeal temperature monitoring may be used for hypoxic perinatal brain injury.3
May be used in the post-resuscitation period, in traumatic brain injury with high intracranial pressure, in the perioperative setting during various surgical procedures (eg, vascular surgery for spinal cord protection and overall neuroprotection) and for various other indications.4
Hypothermia can also be classified as mild, moderate or severe:
Mild hypothermia (32-35°C): associated with lethargy, confusion, shivering, loss of fine motor co-ordination.
Moderate hypothermia (28-32°C): associated with delirium, slowed reflexes.
Severe hypothermia (below 28°C): associated with very cold skin, unresponsive, coma, difficulty breathing, abnormal heart rhythms.
Risk factors
People most likely to experience hypothermia include:
The very elderly or the very young.
Those who are chronically ill, especially with cardiovascular disease.
People who are malnourished.
People who are exhausted.
Those intoxicated with alcohol or drugs.
People with cognitive impairment - eg, in Alzheimer's disease.
Those with underlying medical conditions - eg hypothyroidism, stroke, severe arthritis, Parkinson's disease, trauma, spinal cord injuries, and burns.
Hypothermia symptoms (presentation)
Low-reading thermometers, preferably oesophageal, are required. Tympanic thermometers are unreliable in low temperature measurement. Check for localised cold injury.
Hypothermia usually occurs gradually. Common signs include shivering, slurred speech, an abnormally slow rate of breathing, cold and pale skin, fatigue, lethargy and apathy. A depressed level of consciousness is the most common feature of hypothermia.
The patient is cold to touch and appears grey and cyanotic.
Vital signs (pulse rate, respiratory rate and blood pressure) are variable. Severe depression of respiratory rate and heart rate may result in signs of respiratory and cardiac activity being easily missed.
Differential diagnosis
Cerebrovascular accident.
Drug toxicity: barbiturate, benzodiazepine, cocaine.
Investigations
Monitor for complications - eg, blood gases, FBC, electrolytes, electrocardiogram (ECG) monitoring.
Coagulation studies: disseminated intravascular coagulation may occur.
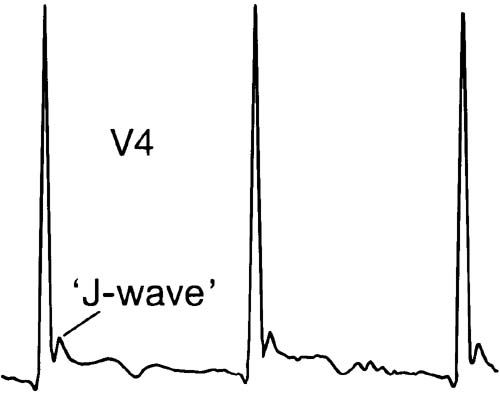
ECG:
May show prolonged PR, QRS and QT intervals, and atrial or ventricular arrhythmias. As the body core temperature decreases, sinus bradycardia tends to give way to atrial fibrillation followed by ventricular fibrillation and finally asystole.
The length and height of the respective QT-interval prolongation and characteristic J waves are often proportional to the degree of hypothermia.
Corrected QRS/QT has been shown in animal studies to have potential as a novel biomarker for predicting risk of hypothermia-induced cardiac arrest.5
HYPOTHERMIA ECG
CXR: aspiration pneumonia and pulmonary oedema are common.
Consider any underlying or associated problems - eg, CT scan for possible head injury.
Treatment for hypothermia (management)
This is directed at re-warming, careful patient monitoring and treatment of complications such as cardiac arrhythmias.
The patient is given warmed, humidified oxygen, and heated intravenous saline, and is surrounded by warmed blankets or heat lamps.
Aggressive management of temperature with faster rather than slow re-warming has been shown to improve the outcome.
Initial management
Immediate attention to airway, breathing and circulation. Initiation of cardiopulmonary resuscitation may be required.6
Administer oxygen via a bag reservoir device.
Establish intravenous access.
Prevent heat loss by removing the patient from the cold environment and replacing wet, cold clothing with warm blankets.
If the person is alert and can easily swallow, then give warm, sweetened, non-alcoholic fluids.
Management in hospital
The patient should ideally be managed in a critical care setting. Attempts to re-warm the patient actively should not delay transfer to a critical care setting.
Assess for and treat any associated disorders - eg, diabetes, sepsis, drug or alcohol ingestion, or occult injuries.
Blood investigations: FBC, electrolytes, blood glucose, alcohol, toxin screen, creatinine, amylase and blood cultures.
Cardiac monitoring: dysrhythmias, changes of hyperkalaemia; J waves are pathognomonic of hypothermia:
Cardiac output falls proportionately to the degree of hypothermia and cardiac irritability begins at about 33°C. Ventricular fibrillation becomes increasingly more common as the temperature falls below 28°C, and at temperatures below 25°C, asystole can occur.
Cardiac drugs and defibrillation are not usually effective in the presence of acidosis, hypoxia and hypothermia. These treatments should usually be reserved until the patient is warmed until at least 28°C.
Cardiopulmonary bypass has been used in patients with severe hypothermia. Patients presenting in cardiac arrest from accidental hypothermia may also be re-warmed effectively using thoracic lavage.
Oxygen:
Administer 100% oxygen while the patient is being re-warmed.
Arterial blood gases are probably best interpreted uncorrected, ie the blood should not be warmed to 37°C which is what most analysers automatically do 7, and those values used as guides to administering sodium bicarbonate and adjusting ventilator parameters during re-warming and resuscitation.
Re-warming technique:
Depends on the patient's temperature, response to simple measures and the presence of any injuries.
Mild and moderate exposure: passive external re-warming in a warm room, using warm blankets, clothing and warmed intravenous fluids.
Severe hypothermia: may require core re-warming methods that may include invasive surgical re-warming techniques - eg, peritoneal lavage, A-V re-warming or cardiopulmonary bypass.
Haemodialysis (HD) is a safe re-warming therapy for moderate and severe hypothermia in the absence of circulatory arrest.8
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) provides an efficient re-warming method with complete cardiopulmonary support. The use of VA-ECMO for this indication has greatly improved the vital and functional prognosis of patients.9
Determination of death can be very difficult in the hypothermic patient. Patients who appear to have suffered a cardiac arrest or death as a result of hypothermia should not be pronounced dead until they are re-warmed (eg, to 35°C; don't have to reach 37°C).
Complications
Cardiovascular: cardiac arrhythmias, hypotension (due to marked vasodilatation when re-warming), intravascular thrombosis.
Respiratory: pneumonia, pulmonary oedema.
Abdominal: pancreatitis, peritonitis, gastrointestinal bleeding, acute tubular necrosis.
Neurological: cognitive decline, memory impairment, judgment impairment, ataxia, dysarthria
Severe hypothermia eventually leads to cardiac failure and respiratory failure, and then death.10
There is a well-recognised association between undesirable hypothermia and negative outcomes in connection with trauma and surgery; however, mild induced hypothermia to ≥33°C does not seem to be associated with either decreased total haemostasis or increased bleeding risk.11
Prognosis
The prognosis depends on the severity and nature of the cause.
Most people tolerate mild hypothermia, which is not associated with significant morbidity or mortality.
Overall mortality then increases with the degree of hypothermia.
Extracorporeal life support has revolutionised re-warming of the haemodynamically unstable patient, with survival rates of up to 100%.12
Preventing hypothermia
Perioperatively there are a range of measures to prevent hypothermia, including covering, forced-air warming devices and warming of intravenous and irrigation fluids used during the procedure.1
The elderly are at particular risk; surveillance by carer and good neighbour is essential.
Heating and insulation grants can make a difference if easy to apply for, but the extra heating allowance is only paid retrospectively.
Even in summer, wet clothing (increases heat loss by 5-10 times) and wind can result in rapid loss of body heat.
To reduce the risk of hypothermia:
Avoid excessive alcohol consumption.
Wear a hat or other protective covering to prevent body heat from escaping from your head, face and neck.
Cover hands with mittens instead of gloves. Mittens are more effective than gloves because mittens keep the fingers in closer contact with one another.
Avoid activities that cause excessive sweating.
Wear loose-fitting, layered, lightweight clothing. Outer clothing made of tightly woven, water-repellent material is best for wind protection. Wool, silk or polypropylene inner layers hold more body heat than cotton.
Stay as dry as possible.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Rathjen NA, Shahbodaghi SD, Brown JA; Hypothermia and Cold Weather Injuries. Am Fam Physician. 2019 Dec 1;100(11):680-686.
- Yi J, Lei Y, Xu S, et al; Intraoperative hypothermia and its clinical outcomes in patients undergoing general anesthesia: National study in China. PLoS One. 2017 Jun 8;12(6):e0177221. doi: 10.1371/journal.pone.0177221. eCollection 2017.
- Alfonsi P, Bekka S, Aegerter P; Prevalence of hypothermia on admission to recovery room remains high despite a large use of forced-air warming devices: Findings of a non-randomized observational multicenter and pragmatic study on perioperative hypothermia prevalence in France. PLoS One. 2019 Dec 23;14(12):e0226038. doi: 10.1371/journal.pone.0226038. eCollection 2019.
- Hypothermia: prevention and management in adults having surgery; NICE Clinical Guideline (December 2016)
- Naseerullah FS, Murthy A; Hypothermia as a forgotten sign of prolonged severe hypoglycaemia. BMJ Case Rep. 2018 Aug 29;2018. pii: bcr-2018-225606. doi: 10.1136/bcr-2018-225606.
- Therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic perinatal brain injury, NICE Interventional Procedure Guideline, May 2010
- Therapeutic hypothermia following cardiac arrest; NICE Interventional Procedure Guideline, March 2011
- Dietrichs ES, Tveita T, Myles R, et al; A novel ECG-biomarker for cardiac arrest during hypothermia. Scand J Trauma Resusc Emerg Med. 2020 Apr 10;28(1):27. doi: 10.1186/s13049-020-00721-0.
- Adult Advanced Life Support; Resuscitation Council (UK) Guidelines (2015 - last updated May 2021)
- Arterial Blood Gas in Hypothermia; C Nickson
- Murakami T, Yoshida T, Kurokochi A, et al; Accidental Hypothermia Treated by Hemodialysis in the Acute Phase: Three Case Reports and a Review of the Literature. Intern Med. 2019 Sep 15;58(18):2743-2748. doi: 10.2169/internalmedicine.1945-18. Epub 2019 Jun 7.
- Ledoux A, Saint Leger P; Therapeutic management of severe hypothermia with veno-arterial ECMO: where do we stand? Case report and review of the current literature. Scand J Trauma Resusc Emerg Med. 2020 Apr 21;28(1):30. doi: 10.1186/s13049-020-00723-y.
- Duong H, Patel G; Hypothermia.
- Kander T, Schott U; Effect of hypothermia on haemostasis and bleeding risk: a narrative review. J Int Med Res. 2019 Aug;47(8):3559-3568. doi: 10.1177/0300060519861469.
- Avellanas Chavala ML, Ayala Gallardo M, Soteras Martinez I, et al; Management of accidental hypothermia: A narrative review. Med Intensiva. 2019 Dec;43(9):556-568. doi: 10.1016/j.medin.2018.11.008. Epub 2019 Jan 22.
About the authorView full bio

Dr Philippa Vincent, MRCGP
General Practitioner, Medical Author
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent is an NHS GP working in North London.
About the reviewerView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 22 Dec 2027
23 Dec 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
More in history and examination
- Abdominal distension and bloating
- Abdominal examination
- Ambulatory blood pressure monitoring
- Anaemia of chronic disease
- Catheterising bladders
- Centile charts and assessing growth
- Complex regional pain syndrome
- Depression
- Flatulence and wind
- Hepatomegaly
- High-altitude illness
- Hyperhidrosis
- Lower urinary tract symptoms in men
- Myalgic encephalomyelitis
- Night terrors and parasomnias
- Painful foot
- Rheumatological history, examination and investigations
- Toe and finger clubbing
- Tourette syndrome and other tic disorders
- Voiding difficulties