Osteoarthritis
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Doug McKechnie, MRCGPLast updated 21 Nov 2022
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Osteoarthritis article more useful, or one of our other health articles.
In this article:
Continue reading below
What is osteoarthritis?
Osteoarthritis (OA) is a clinical syndrome of joint pain accompanied by varying degrees of functional limitation and reduced quality of life. It is the most common form of arthritis and one of the leading causes of pain and disability worldwide. The most commonly affected peripheral joints are the knees, hips and small joints of the hands.1
OA is characterised by localised loss of cartilage, remodelling of adjacent bone and associated inflammation. A variety of traumas may trigger the need for a joint to repair itself. OA includes a slow but efficient repair process that often compensates for the initial trauma, resulting in a structurally altered but symptom-free joint. However, in some people, because of either overwhelming trauma or compromised repair, symptomatic OA eventually presents. There is a great deal of variation in clinical presentation and outcome seen between different people, and also at different joints in the same person. Symptoms of OA often fluctuate over time, and flares are common.1
Epidemiology2
Back to contentsOA is one of the most common chronic diseases, with an estimated overall prevalence in the general adult population of 11% for hip OA and 24% for knee OA, respectively.
OA is age-related, with manifestations often not occurring until middle age.
Risk factors3
Genetic factors:
Heritability estimates for hand, knee and hip OA are about 40-60%.
The responsible genes are largely unknown.
Constitutional factors:
Ageing.
Female sex.
Obesity.
High bone density - risk factor for development of OA.
Low bone density - risk factor for progression of knee and hip OA.
Local, largely biomechanical risk factors:
Joint injury.
Occupational and recreational stresses on joints.
Reduced muscle strength.
Joint laxity.
Joint malalignment.
Continue reading below
Presentation
Back to contentsA diagnosis of OA can be made clinically without investigations if a person:1
Is aged 45 years or over; and
Has activity related joint pain; and
Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30 minutes.
Acute flares of symptoms are common, presenting with increases in pain severity and sometimes joint swelling, inflammation and stiffness,4 lasting from days to weeks.
Symptoms
Joint pain that is exacerbated by exercise and relieved by rest. Rest and night pain can occur in advanced disease. Knee pain due to OA is usually bilateral and felt in and around the knee. Hip pain due to OA is felt in the groin and anterior or lateral thigh. Hip OA pain can also be referred to the knee and, in males, to the testicle on the affected side.
Reduced function and participation restriction.
Signs
Reduced range of joint movement.
Pain on movement of the joint or at extremes of joint movement.
Joint swelling/synovitis (warmth, effusion, synovial thickening).
Periarticular tenderness.
Crepitus.
Absence of systemic features such as fever or rash.
Bony swelling and deformity due to osteophytes - in the fingers this presents as swelling at the distal interphalangeal joints (Heberden's nodes - see image below) or swelling at the proximal interphalangeal joints (Bouchard's nodes).
Heberden's and Bouchard's nodes

© Drahreg01, CC BY-SA 3.0, via Wikimedia Commons
Joint instability.
Muscle weakness/wasting around the affected joint.
Investigations
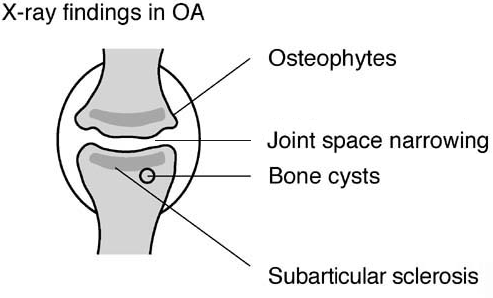
Back to contentsClinical examination: diagnosis is usually based on clinical examination; X-rays are not recommended for routine use unless the diagnosis is in doubt.1
Plain X-rays: when disease is advanced it can be seen on plain X-rays. The diagnostic features that can be seen on X-ray are shown below:
Osteoarthritis X-ray diagram
Body weight and body mass index: should be recorded.
MRI: may be useful to distinguish other causes of joint pain, such as when ligamentous or cartilaginous pathologies are suspected.
Blood tests: are normal in OA. Consider checking baseline FBC, creatinine and LFTs before starting a patient on non-steroidal anti-inflammatory drugs (NSAIDs).
Joint aspiration: may be considered for swollen joints to exclude other causes such as septic arthritis and gout. See the separate Joint Injection and Aspiration article.
Continue reading below
Differential diagnosis3
Back to contentsKnee OA: prepatellar bursitis, meniscal tears, cruciate ligament tears, referred pain from the hip or spine.
Hip OA: greater trochanteric pain syndrome, iliotibial band syndrome, osteonecrosis of the hip, referred pain from the knee or spine.
OA of any joint: fracture of the bone adjacent to the joint (with history of trauma), pseudogout, psoriatic arthritis, septic arthritis, viral arthritis, reactive arthritis, rheumatoid arthritis, gout, malignancy (including bony metastases), connective tissue disease, seronegative arthritis such as ankylosing spondylitis, referred pain, and medical conditions presenting with arthropathy (such as sarcoidosis and infective endocarditis).
Management1
Back to contentsHolistic approach to assessment and management
The effect of OA on a person's function, quality of life, occupation, mood, relationships and leisure activities should be assessed. Consider:
Current thoughts and beliefs - their concerns, expectations, knowledge about OA.
Their support network - ascertain whether there is a carer and, if so, how the main supporter is coping (their ideas, concerns and expectations).
Current mood (screen for depression) - determine whether there is any other stress.
Pain assessment - ask what the patient has tried, including any drugs used (dose, side-effects, timing). Ask whether there are other treatable sources of pain (eg, periarticular pain, trigger finger, ganglion or bursitis). Enquire whether a chronic pain syndrome has developed.
Promote function and reduce adverse effects on activities and sleep; referral to physiotherapy and/or occupational therapy may be indicated.
Consider any comorbidities that may affect choice of treatment or fitness for surgery. Ask whether the patient is prone to falls - and whether this can be minimised.
Any treatments or interventions that require monitoring.
Patients' ability to seek help themselves.
Patients' occupation and activities.
The severity of symptoms and functional limitation.
Core treatments
People with OA should be advised that therapeutic exercise and weight management (if appropriate) are the core treatments for OA. Key treatments for OA include:1
Education, advice and access to information: both oral and written information should be provided.
Exercise: should be encouraged in all people with OA, regardless of their age, comorbidity, pain or disability. This should include exercise for general aerobic fitness and local muscle strengthening. As well as helping weight loss, exercise itself will help to build muscle strength and endurance and can lead to reduced pain and improved joint function.5 Physiotherapy and supervised therapeutic exercise may be useful.
Weight loss advice: if the patient is overweight/obese. This will reduce the load on their joints and help to improve pain. Any amount of weight loss is likely to improve symptoms.
The use of local heat or cold (thermotherapy) can be considered as an adjunct to core treatments, and is frequently used, although high-quality evidence to support its use is lacking.6
Aids and devices:
Advice on appropriate footwear (including shock-absorbing properties) as part of core treatments for people with lower-limb OA.
For patients with biomechanical joint pain or joint instability, insoles/braces/joint supports/tape/splints can be considered as an adjunct to their core treatments, if such devices are required to allow them to perform therapeutic exercise, and the addition of these is likely to improve movement and function.
Assistive devices (eg, walking sticks and tap turners) should be considered as adjuncts to core treatments for people with OA who have specific problems with activities of daily living.
Drug treatments1
Paracetamol and/or topical NSAIDs are reasonable first-line options.3 Paracetamol is suitable for occasional short-term pain relief, or where other pharmacological options are contra-indicated, not tolerated, or ineffective. However, evidence suggests that paracetamol produces minimal, if any, improvement in pain and function in OA.7 1 .
Topical treatments:
Topical NSAIDs may be useful for hand and knee OA and can be considered for OA of other joints.
Topical capsaicin can be used for hand and knee OA.
If paracetamol and/or topical NSAIDs are ineffective, oral NSAIDs should be offered at the lowest effective dose for the shortest possible time, taking into account the risk of GI, renal, liver and cardiovascular toxicity and any relevant risk factors the patient has (such as age, pregnancy, comorbidity and current medications).
Topical NSAIDs should be stopped if oral NSAIDs are used.3
Gastroprotective treatment (such as proton-pump inhibitors) should be offered alongside oral NSAIDs.1
Standard NSAIDs or COX-2 inhibitors can be used first-line.
In people with risk factors for cardiovascular disease, and all elderly people, ibuprofen up to 1200 mg daily or naproxen up to 1000 mg daily is preferred.8
COX-2 inhibitors, diclofenac and high-dose ibuprofen are contra-indicated in people with cardiovascular disease.8
NSAIDs should ideally be avoided in people with severe renal impairment (eGFR <30 mL/min/1.73 m2).
Concomitant use of NSAIDs with low-dose aspirin should be avoided; alternatives to oral NSAIDs should be sought if low-dose aspirin treatment needs to continue.
Weak opioids may be used infrequently for short-term pain relief if all other options are ineffective or unsuitable. The risks and benefits should be carefully considered, particularly in older people.
Strong opioids should not be used for OA.1
Compared with placebo, glucosamine, chondroitin and their combination do not reduce joint pain or have an impact on narrowing of joint space.9 Glucosamine is not recommended for the treatment of OA.1
Intra-articular injections:
Intra-articular corticosteroid injections can be used when other pharmacological treatments are ineffective or unsuitable, or to support therapeutic exercise. Patients should be aware that these only offer short-term relief (2 to 10 weeks).1
Do not offer intra-articular hyaluronan injections for the management of OA.
Topical herbal treatments: although topical capsaicin has been recommended as a treatment option, there is otherwise not a great deal of evidence from studies to show that herbal remedies are effective:10
Arnica gel probably improves symptoms as effectively as a gel containing an NSAID.
Comfrey extract gel probably improves pain.
There has been no strong evidence for capsicum extract gel.
Referral for consideration of joint surgery
Ensure that the person has been offered at least the core (non-surgical) treatment options before referral.
Referral decisions should be based on clinical assessment, rather than numerical scoring tools to score disease severity.
Arthroscopic lavage and debridement should not be offered as a treatment for OA.
Consider referral for joint surgery for people with hip, knee, or shoulder OA who experience joint symptoms (pain, stiffness and reduced function) that have a substantial impact on their quality of life, and where non-surgical treatment is ineffective or unsuitable.
Refer for consideration of joint surgery before there is prolonged and established functional limitation and severe pain.
Patient-specific factors (including age, sex, smoking, obesity and comorbidities) should not be barriers to referral for joint surgery, although the potential impact of these on the risks of joint replacement surgery should be discussed when considering referral.
Emerging treatments
Magnetic resonance therapy (MRT) for knee osteoarthritis uses a device placed over the knee joint to generate electromagnetic fields targeted at cartilaginous tissue, with the aim of promoting joint repair and improving symptoms. The 2021 interventional procedures review from the National Institute for Health and Care Excellence (NICE) found that, whilst there were no major safety concerns, evidence of efficacy was inadequate. NICE therefore recommends that MRT should only be used as part of a research study.11
Genicular artery embolisation (GAE) aims to reduce blood flow to neovascularities supplying the arthritic knee joint, thereby reducing inflammation and nociceptive nerve growth. NICE's 2021 interventional procedures guidance found no major short-term safety concerns, but that evidence on efficacy and long-term safety was lacking. NICE therefore recommends that GAE for pain in OA is only performed in research studies.12
Prognosis3
Back to contentsOsteoarthritis is not always progressive and does not inevitably lead to increasing pain and functional impairment:
Hand involvement has a good prognosis. Interphalangeal joint involvement usually becomes asymptomatic after a few years. Osteoarthritis of the first carpometacarpal (CMC) joint has a poorer prognosis.
Hip involvement has a poorer prognosis than hand or knee. A significant proportion of people require hip replacement within five years of diagnosis.
Knee involvement has a variable prognosis. Symptoms may improve spontaneously, remain stable, or progressively worsen, with structural changes on X-ray, which eventually require joint surgery.
Prevention
Back to contentsWeight control.
Increasing physical activity.
Avoiding injury.
Improving education about OA, including increased use of expert patient programmes.
Optimal management of symptoms by GPs to reduce the prevalence of disability due to OA.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Maricar N, Callaghan MJ, Felson DT, et al; Predictors of response to intra-articular steroid injections in knee osteoarthritis--a systematic review. Rheumatology (Oxford). 2013 Jun;52(6):1022-32. doi: 10.1093/rheumatology/kes368. Epub 2012 Dec 22.
- Day RO, Graham GG; Non-steroidal anti-inflammatory drugs (NSAIDs). BMJ. 2013 Jun 11;346:f3195. doi: 10.1136/bmj.f3195.
- Platelet-rich plasma injections for osteoarthritis of the knee; NICE Interventional Procedure Guidance, May 2014
- Scarpignato C, Lanas A, Blandizzi C, et al; Safe prescribing of non-steroidal anti-inflammatory drugs in patients with osteoarthritis - an expert consensus addressing benefits as well as gastrointestinal and cardiovascular risks. BMC Med. 2015 Mar 19;13(1):55. doi: 10.1186/s12916-015-0285-8.
- Osteoarthritis; NICE Quality Standard, June 2015 - updated October 2022
- da Costa BR, Pereira TV, Saadat P, et al; Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: network meta-analysis. BMJ. 2021 Oct 12;375:n2321. doi: 10.1136/bmj.n2321.
- Osteoarthritis in over 16s: diagnosis and management; NICE guideline (October 2022)
- EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis; Annals of Rheumatic Disease (April 2013)
- Osteoarthritis; NICE CKS, August 2022 (UK access only)
- Parry EL, Thomas MJ, Peat G; Defining acute flares in knee osteoarthritis: a systematic review. BMJ Open. 2018 Jul 19;8(7):e019804. doi: 10.1136/bmjopen-2017-019804.
- Fransen M, McConnell S, Harmer AR, et al; Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2015 Jan 9;1:CD004376. doi: 10.1002/14651858.CD004376.pub3.
- Brosseau L, Yonge KA, Robinson V, et al; Thermotherapy for treatment of osteoarthritis. Cochrane Database Syst Rev. 2003;(4):CD004522.
- Leopoldino AO, Machado GC, Ferreira PH, et al; Paracetamol versus placebo for knee and hip osteoarthritis. Cochrane Database Syst Rev. 2019 Feb 25;2:CD013273. doi: 10.1002/14651858.CD013273.
- NSAIDs - prescribing issues; NICE CKS, April 2020 (UK access only)
- Wandel S, Juni P, Tendal B, et al; Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ. 2010 Sep 16;341:c4675. doi: 10.1136/bmj.c4675.
- Cameron M, Chrubasik S; Topical herbal therapies for treating osteoarthritis. Cochrane Database Syst Rev. 2013 May 31;5:CD010538. doi: 10.1002/14651858.CD010538.
- Magnetic resonance therapy for knee osteoarthritis; NICE Interventional procedures guidance, August 2021
- Genicular artery embolisation for pain from knee osteoarthritis; NICE Interventional procedures guidance, October 2021
Continue reading below
About the authorView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 20 Nov 2027
21 Nov 2022 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free