Immune thrombocytopenic purpura
ITP
Peer reviewed by Dr Rosalyn Adleman, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 16 Mar 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In immune thrombocytopenic purpura, antibodies are made against platelets. Once the antibodies have attached to platelets, the platelets do not work so well.
At a glance
Immune thrombocytopenic purpura (ITP) is an autoimmune disorder where the body attacks its own platelets.
Platelets are blood components that help blood clot.
Symptoms can include bruising, a purple-red rash (purpura), and nosebleeds.
ITP can affect both children and adults, but it often behaves differently in each group.
Diagnosis is made with a blood test that shows a lower than normal number of platelets.
Most children with ITP will not need treatment, and the condition often resolves on its own.
Adults with ITP may require treatment with steroids or other medicines, or sometimes surgery.
What is immune thrombocytopenic purpura?
Immune thrombocytopenic purpura (ITP) is an autoimmune disorder. In autoimmune disorders your body makes proteins called antibodies which damage another part of your body. In ITP the antibodies are made against platelets.
Once the antibodies have attached to platelets, the platelets do not work so well. They are also removed more quickly by the spleen because they are abnormal.
It is called 'immune' because it is now known that a problem with the immune system is the cause.
Thrombocytopenic, or thrombocytopenia, means not having enough platelets.
Purpura is a purple-red rash. It is caused by tiny bleeds under the skin.
ITP is quite different in children and adults and should be considered separately.
Understanding platelets
Platelets are tiny components of the blood which help blood to clot when we injure ourselves. They are also known as thrombocytes. They are made inside bone, in the bone marrow.
They are released into the bloodstream and travel through the body for about seven days, before they are removed by the spleen. The spleen is an organ that lies at the top of the tummy (abdomen) under the ribs on the left-hand side.
The spleen
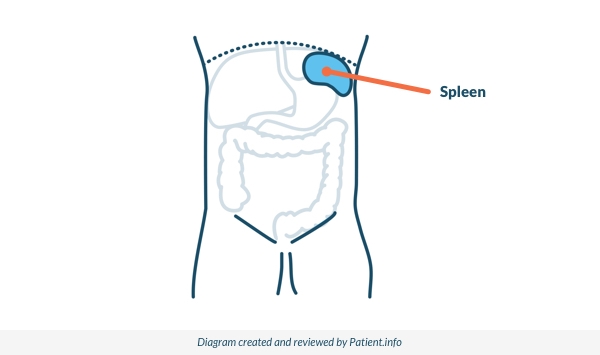
A normal number of platelets is between 150 and 400 x 109 per litre. This is found by a blood test. If you have too many platelets, your blood will clot too easily. If you do not have enough platelets, you may bruise and bleed more easily than usual.
Immune thrombocytopenic purpura in children
ITP occurs in about 5 of every 100,000 children. It is most common in children around the age of 5 or 6 years, but it can occur at any age.
Symptoms of ITP in children
Most children will not have any symptoms of ITP.
Those who do develop symptoms have bruising or a purple or red rash - purpura. There may be tiny red spots, or larger areas of bruising or rash. This usually appears over 1-2 days.
Some have nosebleeds. Older girls may have heavier periods.
The condition often occurs about 2-3 weeks after an infection (often a common viral infection). Occasionally, it follows immunisation. The symptoms often disappear over 6-8 weeks, and by six months in most cases.
Very occasionally, it causes severe bleeding which requires emergency treatment.
The platelet levels in about 1 or 2 in 10 affected children do not return to normal after a year. This is then called chronic ITP, which means it is persistent. However, many of these children will never need any treatment.
So, what seems to happen in children with ITP is that the immune system is triggered to produce antibodies against the platelets by an infecting virus or other germ. In most cases, this is a temporary immune reaction that lasts several weeks only, and then symptoms go. But, in a few cases, the immune system continues to be faulty and the condition becomes long-standing.
How is ITP diagnosed in children?
ITP is diagnosed by a blood test called a full blood count. This test shows that there are fewer platelets than normal. The laboratory will also have a look at the blood under a microscope.
Sometimes different tests will be needed to make sure that the low number of platelets is not due to another of the possible causes. Rarely, this involves taking a sample of bone marrow. This is not needed if the blood count and symptoms are typical of ITP.
What is the treatment for ITP in children?
In addition to any treatment that is required, your child will need to have regular blood tests and specialist review. If they have an injury or are involved in an accident you will be advised to take them to your local hospital emergency department for review. If the disease is severe then the treatments outlined below may be considered.
Children with ITP may be advised to avoid contact sports. This is because they may get more bleeding than normal from minor injuries. PE teachers or those looking after a child with ITP should be aware.
Children with ITP should not take medicines such as aspirin or ibuprofen, as these can also increase the risk of bleeding. You should contact a doctor urgently if your child has:
A nosebleed which will not stop despite pinching the nose after 30 minutes.
Prolonged bleeding from the gums.
Blood in the poo (stools) or urine.
A heavy blow to the head, especially if the child is unwell afterwards in any way.
Persistent or severe headache.
Sickness (vomiting).
Unexplained drowsiness.
Most children will not need treatment, even if the number of platelets is very low. The decision to treat is usually based on whether your child has serious bleeding or severe bruising and purpura.
This is because some children can have very low platelet counts but still not have any bleeding problems. If the symptoms are mild, usually there will be no need for treatment.
Your child may need to have the full blood count repeated on a few occasions to check that the platelet numbers are stable and that the rest of the blood cell counts are remaining normal.
If your child has bleeding and more severe bruising or purpura, treatment may be considered. The aim of treatment is to improve symptoms and increase the number of platelets.
If treatment is needed then the decision on what treatment to use can be difficult. This is because there have not been many studies testing the treatments against each other. The options for treatment include:
Prednisolone
This is often the first type of treatment tried. It is a steroid medication and is taken as syrup or tablets. This may be given as a high dose over a short period of time (four days) or as a lower dose for a longer time (two weeks). Prednisolone has been shown to increase the number of platelets quickly in about 3 in 4 children with ITP.
Other steroid options
High-dose methylprednisolone or high-dose dexamethasone. These are other types of steroid medicines that have also been shown to be effective in differing degrees. These are less often used now than they used to be.
Intravenous immunoglobulin (IVIg)
This is an injection of a protein into the bloodstream and has been shown to work well in about 8 in 10 children in increasing the number of platelets.
It is not usually used as the first option because it involves an injection. It can also cause quite a lot of side-effects and is quite expensive. It may be used as an emergency treatment if your child has severe bleeding or needs surgery.
Anti-D immunoglobulin
This is another type of protein that is also effective and causes fewer side-effects than IVIg. It can only be given to children whose blood group is rhesus (RhD) positive.
Platelet transfusions
In a life-threatening situation your child may be given a transfusion of platelets at the same time as being treated with steroids and IVIg.
This only helps to increase the number of platelets for a short time. The transfused platelets are also attacked by the antibody that the body has produced and are destroyed by the spleen.
Other medicines
A number of other medicines may be used. These are not routinely recommended, as not enough information is known yet about their use and side-effects. One such medicine is called rituximab. This is used more in adults than in children at the moment in the UK.
Surgery to remove the spleen (splenectomy)
This is very rarely done in children with ITP. It is only really considered as an option if your child has life-threatening bleeding or severe chronic disease that is affecting their day-to-day functioning.
What is the outlook for ITP in children?
Childhood ITP usually resolves within a few weeks or months, but in a minority of children, ITP does not resolve quickly and these children develop chronic ITP.
Chronic ITP in children
Chronic ITP (low platelet count persisting for longer than 12 months) occurs in about 1-2 in every 10 children with ITP. Studies have shown that older age of the child, a higher platelet count and having no preceding infection increase the risk of chronic ITP.
In chronic ITP, recovery occurs within five years of diagnosis in about 1 in 2 children.
Immune thrombocytopenic purpura in adults
ITP occurs in about 3 in 100,000 adults every year. It is more common in women than in men between the ages of 30 and 60 years. At other ages, it is just as common in men as it is in women.
Symptoms of ITP in adults
In adults, ITP comes on gradually and does not usually follow a viral illness. It is not really known what causes the disease. The symptoms may vary a lot. You may have no symptoms, purpura, mild bruising or bleeding, or severe bleeding. Unlike ITP in children, most adults with ITP will continue to have a low number of platelets indefinitely. This is called chronic ITP.
How is ITP diagnosed in adults?
Because most adults with ITP do not have any symptoms, ITP is usually diagnosed on a routine blood test that has been done for other reasons. The full blood count shows a lower number of platelets than normal. The laboratory will also look at your blood under a microscope.
Sometimes (if your symptoms are unusual) a sample from your bone marrow may be necessary. Low platelet numbers can be due to other causes such as medication, viral infections or other diseases. It may be necessary for you to have some additional tests to rule out these other conditions.
Investigations also include tests for Helicobacter pylori. If this test is positive then treatment to remove Helicobacter pylori has been shown to improve the platelet count for many people with ITP.
What is the treatment for ITP in adults?
Most adults with ITP do not require active treatment, unless they have significant symptoms or need to undergo surgery for any reason, including dental work. It is important to have adequate platelet levels before surgery, in order to reduce the risk of severe bleeding during the operation.
Steroids
If treatment is needed then the first treatment that tends to be used in an adult with ITP is usually steroids. Sometimes steroids are used along with injections of IVIg. Both of these treatments increase the platelet count in many people. Usually though, this improvement is only temporary and the platelet numbers return to a low level after a few weeks. Anti-D immunoglobulin can also be used in adults and has been shown to increase platelet numbers effectively.
Splenectomy
Surgery to remove the spleen (splenectomy) is used more often in adults than in children. It is more likely to result in a longer-lasting normal number of platelets. About 2 in 3 people with ITP who have a splenectomy will have a normal number of platelets afterwards for at least five years.
However, splenectomy is not without possible complications. As the spleen is responsible for fighting certain types of infection, people who have had their spleen removed are more at risk of some serious infections.
For this reason, you will need to have some extra vaccinations and may be advised to take antibiotics every day. See the separate leaflet called Preventing Infection after Splenectomy for more details.
Other treatments
If the above treatments do not work, there are several other options. For example, you may be given another trial of steroids or IVIg. Other treatments that may be used include danazol and medications to suppress the immune system, such as azathioprine or ciclosporin.
A medicine called rituximab has also produced good responses. Other new treatments include medicines which help you make more platelets.
These are called romiplostim and eltrombopag. They may be used if you are having severe bleeding, and if other treatments have not been helpful.
Fostamatinib for immune thrombocytopenia
Fostamatinib is usually used at the same stage of treatment as rituximab - for adults with long-term symptoms which have not responded to other treatments. The National Institute for Health and Care Excellence (NICE) has looked at the evidence for this medicine and advised that it can be used when other medicines have been tried.
Specifically, these other medicines would be thrombopoietin receptor agonists (TPO-RA). They work by increasing the number of platelets in the blood (cells that help the blood to clot). If these medicines don't work or they are not suitable for you, then fostamatinib can be used. Evidence has shown that it is better than rituximab at increasing the number of platelets in the blood.
What if I am pregnant?
A low number of platelets in pregnancy is quite common. It can be difficult to know if your platelet count is low due to the pregnancy or due to ITP. If you have no symptoms and the number of platelets is not too low, you may just be monitored.
If the number of platelets needs to be increased then steroids or IVIg can be used. ITP will not make a difference to which type of delivery you have.
It is very unlikely that your low number of platelets will cause any problems to your newborn baby. After they have been born, their platelet level will be checked and, if it is low, they will be monitored carefully. If they need treatment, IVIg can be used.
What is the outlook for ITP in adults?
In adults, the outlook (prognosis) is variable depending on the severity of symptoms. Most people do not need any treatment. If treatment is needed, the response to treatment varies from person to person.
Patient picks for Immune system disorders

Allergies, blood and immune system
The immune system
This leaflet gives a brief overview of the immune system and how it works. A person with a weak immune system might have difficulty fighting off infections. In autoimmune diseases the body is unable to tell what is its own and what is foreign, so it attacks itself. Autoimmune diseases can attack any part of the body - eg, type 1 diabetes (pancreas), multiple sclerosis (brain and nerves), systemic lupus erythematosus (skin and organs). These diseases are managed by the specialist who knows most about the system affected for that person - eg, multiple sclerosis is managed by a neurologist.
by Dr Toni Hazell, FRCGP
Allergies, blood and immune system
Immunosuppression
Immune suppression describes a loss of immune function. It can occur for many reasons, including disease, medication, surgery, age or genetics.
by Dr Philippa Vincent, MRCGP
Frequently asked questions
What is the function of the spleen in ITP?
In ITP, antibodies attach to platelets, making them abnormal. The spleen then removes these abnormal platelets more quickly than usual. This process contributes to the low platelet count seen in ITP.
Are there specific warning signs that indicate a child with ITP needs urgent medical attention?
Yes, you should contact a doctor urgently if your child experiences a nosebleed that doesn't stop after 30 minutes of pinching, prolonged bleeding from the gums, blood in their poo or urine, a heavy blow to the head followed by any unwellness, a persistent or severe headache, sickness (vomiting), or unexplained drowsiness.
What should adults with ITP consider if they need surgery or dental work?
Most adults with ITP do not require active treatment unless they have significant symptoms or need to undergo surgery, including dental work. It is crucial to ensure adequate platelet levels before any surgical procedure to reduce the risk of severe bleeding during the operation.
How common is ITP in children compared to adults?
ITP occurs in about 5 out of every 100,000 children, most commonly around 5 or 6 years of age. In adults, ITP occurs in approximately 3 out of every 100,000 adults annually. It is more common in women aged 30-60, but equally common in men and women at other ages.
Does ITP impact pregnancy or the newborn baby?
A low number of platelets is common in pregnancy, and it can be challenging to determine if it's due to pregnancy or ITP. If platelet levels are not too low and there are no symptoms, monitoring might be sufficient. Steroids or IVIg can be used if platelet levels need to be increased. ITP does not affect the delivery type, and it's very unlikely to cause problems for the newborn baby. The baby's platelet level will be checked after birth, and if low, they will be monitored or treated with IVIg if necessary.
Further reading and references
- Purpura; DermNet NZ
- Nagalla S, Sarode R; Recent advances in understanding and management of acquired thrombocytopenia. F1000Res. 2018 Jan 17;7:68. doi: 10.12688/f1000research.12309.1. eCollection 2018.
- Fostamatinib for treating refractory chronic immune thrombocytopenia; NICE Technology appraisal guidance, October 2022
- Lambert MP, Gernsheimer TB; Clinical updates in adult immune thrombocytopenia. Blood. 2017 May 25;129(21):2829-2835. doi: 10.1182/blood-2017-03-754119. Epub 2017 Apr 17.
- Provan D, Arnold DM, Bussel JB, et al; Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019 Nov 26;3(22):3780-3817. doi: 10.1182/bloodadvances.2019000812.
- Despotovic JM, Grimes AB; Pediatric ITP: is it different from adult ITP? Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):405-411. doi: 10.1182/asheducation-2018.1.405.
- Kim DS; Recent advances in treatments of adult immune thrombocytopenia. Blood Res. 2022 Apr 30;57(S1):112-119. doi: 10.5045/br.2022.2022038.
- Vianelli N, Auteri G, Buccisano F, et al; Refractory primary immune thrombocytopenia (ITP): current clinical challenges and therapeutic perspectives. Ann Hematol. 2022 May;101(5):963-978. doi: 10.1007/s00277-022-04786-y. Epub 2022 Feb 24.
- Yacobovich J, Revel-Vilk S, Tamary H; Childhood immune thrombocytopenia--who will spontaneously recover? Semin Hematol. 2013 Jan;50 Suppl 1:S71-4. doi: 10.1053/j.seminhematol.2013.03.013.
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Rosalyn Adleman, MRCGP
MRCGP
Dr Rosalyn Adleman, is an NHS GP working in north London.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 7 Feb 2028
16 Mar 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in allergies, blood and immune system
- Acute myeloid leukaemia
- Addison's disease
- Anaphylaxis
- Antibody and antigen tests
- Blood glucose test (blood sugar) and HbA1c
- Blood tests to detect inflammation
- Bone marrow biopsy and aspiration
- Bullous pemphigoid
- Chronic myeloid leukaemia
- Coombs test
- Drug allergy
- Full blood count and blood film
- Glucose tolerance test
- Hodgkin's lymphoma
- Liver function tests
- Psoriatic arthritis
- Routine kidney function blood test
- Sickle cell disease
- Thrombophilia
- Vitiligo