Cataracts and cataract surgery
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Laurence KnottLast updated 14 Dec 2021
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Cataracts article more useful, or one of our other health articles.
In this article:
Continue reading below
What are cataracts?
Cataracts are lens opacities. Some are small and do not need treatment but they often become large enough to block light and obstruct vision.
What causes cataracts?
Back to contentsAgeing is the main cause of cataract development in the developed world, although they can also form congenitally and after various forms of injury to the lens. In the developing world other factors contribute, including malnutrition, acute dehydrating illnesses and excess ultraviolet (UV) exposure. Lack of access to treatment makes them a leading cause of sight loss worldwide.
Continue reading below
How common are cataracts? (Epidemiology)1
Back to contentsThe prevalence of cataract increases with age: a systematic review found the pooled prevalence (the prevalence of members of samples pooled together) of any cataract was:
20-39 years - 3.01%.
40-59 years - 16.97%
Over 60 years - 54.38%.
A UK study that randomly sampled 1,547 people of 65 years of age and older found that the prevalence of visually-impairing cataracts was:
71% in people aged over 85 years.
59% in people aged 80-84 years.
42% in people aged 75-79 years.
24% in people aged 70-74 years.
16% in people aged 65-69 years.
Cataracts are uncommon in children.
Globally, cataracts are the world's leading cause of sight loss. About 36 million people worldwide have lost their sight, and in over 12 million of them this is due to cataract.
Risk factors of cataracts2 3
Back to contentsApart from age, the most significant types of cataract risk factors in the developed world are:
Smoking
Diabetes mellitus
Systemic corticosteroids
Other risk factors contributing to cataract formation include:
Eye trauma.
Female gender.
Uveitis.
UV exposure.
Poor nutrition.
Lower socio-economic status.
Smoking and alcohol.
Toxins - eg, drugs of misuse.
Dehydrating illness crises.
Metabolic disorders - eg, galactosaemia in children.
Inflammatory and degenerative eye diseases.
Genetic studies estimate that the heritability of an age-related cataract is around 50%.
Evidence that topical (including inhaled) steroids alone increase the risk of cataract formation is unclear4 5 .
In the developing world the main extrinsic factors are:
Diet (malnutrition).
Acute dehydrating diseases.
Cumulative exposure to sunlight.
In developing countries, cataracts are common in young adults and may be associated with atopy and with diabetes.
Continue reading below
Can cataracts be improved with diet?6
Back to contentsThe development of acquired cataract is principally caused by oxidative damage, which naturally leads to consideration of ameliorating this damage by increasing the amount of antioxidants in the diet. However, no strategy has provided convincing evidence of effectiveness in slowing cataract growth. Current thinking is that it is not so much the content of the diet but the effectiveness of internal systems to transport endogenous antioxidants to the lens. Future research therefore needs to take into account the underlying physiology of how specific nutrients and antioxidants are delivered, taken up and metabolised to maintain and restore antioxidant levels in the different regions of the lens.
Pathophysiology of cataract7 8
Back to contentsThe lens continues to grow after birth, with the new secondary fibres being added as outer layers. New lens fibres are generated from the lens epithelium. Old fibres are not removed.
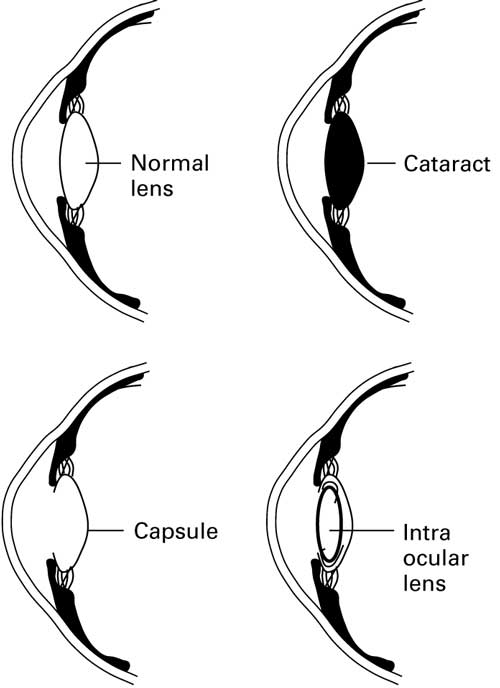
Lens transparency is maintained by many factors, including its microscopic structure and chemistry. The lens has three main parts: the capsule, the epithelium and the fibres. The lens has no nerves, blood vessels, or connective tissue.
The lens capsule is elastic and is composed of collagen.
The lens epithelium, in the anterior portion of the lens between the capsule and the fibres, regulates the homeostasis of the lens and constantly lays down new fibres.
The lens fibres form the bulk of the lens. They are long, thin, transparent cells, arranged lengthwise from the posterior to the anterior poles. They are stacked arranged in concentric layers. They have no nuclei and are composed mainly of crystallins (water-soluble proteins). The transparency of the lens is maintained by the arrangements of these fibres, their lack of intracellular bodies like nuclei, and their cytoskeletons which maintain the architecture.
Transparency is maintained by the structure of the lens proteins and by the way they are stacked, linked and aligned. Disruption of the crystallin fibres will affect the integrity of the carefully composed structure, leading to protein aggregation. Cataracts result from the deposition of aggregated proteins in the lens, causing clouding, light scattering, double vision and obstruction of vision.
A second contributing factor which occurs with ageing is an accumulation of yellow-brown pigment in the lens. This does not affect image sharpness but it affects colour vision and contrast, so may eventually make reading difficult2 .
Cataract symptoms9
Back to contentsWhat are the symptoms of cataracts?
This depends upon the size and location of the opacity and whether one or both eyes are affected. The most consistent presenting features are:
Gradual painless loss of vision.
Difficulties with reading.
Failure to recognise faces.
Problems watching TV.
Diplopia in one eye.
Haloes.
Many cataracts present before they are symptomatic, because they are noticed by an optician at a routine eye exam.
Cataracts are often described by the part of the lens that is particularly affected. This also affects their typical presentation. There are many possible subdivisions but three broad categories are generally described:
Nuclear sclerosis: this cataract is formed by new layers of fibre (added with ageing) compressing the nucleus of the lens. Typical symptoms include:
Gradually reduced contrast.
Reduced colour intensity.
Reading which may be surprisingly good for acuity level.
Difficulty in seeing golf balls, car number plates, etc.
Difficulty in recognising faces.
Cortical: new fibres are added to the outside of the lens, which age and produce cortical spokes. These may not produce symptoms unless on the visual axis or the entire cortex is affected when it is 'mature':
Light scatter from opacities.
Problems with glare when driving, particularly at night.
Difficulty reading.
Daytime activity relatively unaffected as the iris is constricted.
Posterior subcapsular: opacities in the central posterior cortex. This may occur in younger patients and may cause glare ± deterioration in near vision:
Visually disabling in good lighting - less trouble at low light levels when the pupil is dilated.
Difficulty in daytime driving.
Difficulty in reading.
Paediatric cataracts1
These may be:
Congenital : hereditary/genetic, metabolic (eg, galactosaemia), in-utero infection (toxoplasmosis, other, rubella, cytomegalovirus, herpes simplex (TORCH)).
Developmental: genetic, metabolic (eg, galactokinase deficiency).
Acquired: metabolic (eg, diabetes mellitus), traumatic, post-radiotherapy.
The most common cause of congenital cataracts is infection - rubella (the most common), measles, chickenpox, cytomegalovirus, herpes simplex, herpes zoster, poliomyelitis, influenza, Epstein-Barr virus, syphilis and toxoplasmosis. Other causes are metabolic and genetic syndromes.
Signs of cataracts
Opacities can be seen as defects in the red reflex obtained when the ophthalmoscope is held 60 cm from the eye. This is best seen with a dilated pupil.
The lens may appear brown or white when a bright light is shone on the eye.
Check that:
Visual acuity is not improved by viewing test through a pinhole.
The patient can indicate where a light is placed.
Pupillary reactions are normal.
Differential diagnosis
Back to contentsCataract treatment and management2
Back to contentsThere is no proven prevention or medical treatment for a cataract. Modern cataract surgery involves lens extraction and replacement. The technique can be intracapsular or extracapsular, although intracapsular extraction is now rarely performed. Surgical removal of the cataract is the only effective treatment to restore or maintain vision.
In the developed world, cataracts are easily treated before vision is severely impaired. In the developing world, cataracts lead to significant problems of severe visual impairment. This is because most people do not seek advice until the cataract is advanced or the eye has developed lens-induced glaucoma, a painful condition. This is partly due to lack of awareness and partly due to a lack of government or socially funded healthcare in countries where socio-economic conditions are poor. Many countries lack sufficient clinicians to meet demand, particularly in rural areas.
Cataract surgery9 1
There is no absolute threshold of visual acuity at which surgery is indicated. The National Institute for Health and Care Excellence (NICE) advises that the decision to refer a person with a cataract for surgery should be based on a discussion with them that includes: how the cataract affects the person's vision and quality of life; whether one or both eyes are affected; what cataract surgery involves, including possible risks and benefits; how the person's quality of life may be affected if they choose not to have cataract surgery and whether the person wants to have cataract surgery. It states that access to cataract surgery should not be restricted on the basis of visual acuity9 .
Extracapsular lens extraction: manual extraction and phacoemulsification
Extracapsular lens extraction involves removal of the anterior capsule and extraction of the lens nucleus and cortex, either manually via a large incision at the limbus, or after phacoemulsification of the lens via ultrasound via a smaller incision. The posterior capsule is left to support the implanted artificial lens.
Cataract surgery can be performed on a day-case basis, either with a locally injected anaesthetic or even with anaesthetic eye drops. Postoperative care includes the use of topical antibiotics and steroids with avoidance of strenuous activity. Multifocal (non-accommodative) intraocular lenses can be implanted during surgery and provide good vision10 .
Phacoemulsification is the most widely used, safest and most effective extracapsular technique:
A 3 mm diameter incision is made in the sclera
A round hole of approximately 5 mm in diameter is made in the lens capsule.
The hard lens nucleus is liquefied by an ultrasonic probe inserted through the hole, and extracted.
Soft lens fibres are aspirated.
The replacement lens is placed folded into the now empty capsular bag where it unfolds.
The hole usually heals without sutures.
Phacoemulsification involves a smaller incision, with lower complication rates.
Visual recovery is faster following phacoemulsification
Phacoemulsification results in less induced astigmatism
However, manual small incision extracapsular extraction is faster, requires less sophisticated equipment and is less expensive. It remains the preferred technique in many parts of the developing world11 .
The proportion of patients who achieve a corrected visual acuity of better than 6/12 after three months is similar for the two procedures12 .
Intracapsular extraction
This involves removing the lens in its entirety. The lens may be replaced with a plastic lens which may be stitched into place at the sulcus. Previously, patients were often left aphakic after intracapsular cataract surgery. The refractive power of the natural lens in its natural state is about 18 dioptres, so an eye with no lens (aphakic eye) needs very strong glasses. This caused significant visual problems, including objects being apparently nearer than they really are, loss of visual field and a ring of blindness An added problem is that in the developing world such glasses have not always been available.
The intracapsular technique was used widely in the past but has been largely abandoned due to the higher rate of complications and larger incision required, the difficulties of aphakia and the improved availablility of artificial lenses.
Cataract
Complications of cataract surgery13 14 15 16
Back to contentsCataract surgery is a safe and successful procedure in the majority of cases. Poor vision after cataract surgery is generally due to:
Inadequate correction of refractive error postoperatively.
Failure to detect pre-existing eye conditions. Serious co-existing eye conditions such as glaucoma, age-related macular degeneration, diabetic retinopathy and amblyopia are often present in patients requiring cataract surgery.
Surgical complications.
The most common complication is capsular rupture with vitreous loss, which is significant, as it is often associated with a poorer outcome. It also increases the risk of endophthalmitis, which is rare but devastating.
Early complications of cataract surgery
Posterior capsule rupture with or without loss of vitreous (1-3%).
Protruding or broken sutures.
Trauma to the iris.
Wound gape or prolapse of iris (<1%).
Anterior chamber haemorrhage (<1%).
Vitreous haemorrhage (<1%).
Choroidal haemorrhage (<1%).
Endophthalmitis - a devastating but rare condition which occurs in around 0.05-0.1% of cases. Staphylococcus epidermidis is the most common infecting organism17 18 .
Refractory uveitis due to low-grade infection. This can be avoided by intraoperative antibiotic prophylaxis19 .
Late complications of cataract surgery
Posterior capsule opacification - this is a late complication (around 40%) and is the most common finding. Vision can usually be restored with laser capsulotomy.
Cystoid macular oedema, more frequently diagnosed by angiography (1%).
Retinal detachment, which can occur weeks, months or even years later. The lifetime risk is about 1 per 150 operations, more likely in case of high myopia.
Open-angle glaucoma (<1%).
Closed-angle glaucoma (<1%).
Bullous keratopathy (a rare complication).
Increased risk of age-related macular degeneration requiring photodynamic therapy20 .
Dysphotopsias.
Negative and positive dysphotopsias are unwanted optical phenomena occurring after cataract surgery due to intraocular light artefacts reflecting off the IOL21 22 23 . They are the main cause of post-surgical dissatisfaction. Positive dysphotopsia (glare, haloes and starbursts) is largely attributed to edge effects of the implant, whilst negative dysphotopsia appears related to the patient's anatomical structure. Improvements in edge designs have diminished the effects of positive dysphotopsia, which has previously been reported to occur in 12-67% of patients. However, negative dysphotopsia (2.5% of patients) remains poorly understood.
Most dysphotopsias resolve or diminish over time. However, in 0.2 to 1% of patients severe symptoms persist24 . Implantation of a secondary intraocular lens (IOL) can alleviate negative dysphotopsias25 .
Surgical complications are more likely to occur in patients with existing dystrophies, mature cataracts or high ametropia (>6 dioptres of myopia or hypermetropia). Simple scoring systems have been devised to stratify patients into three risk groups. This allows for individualised risk counselling26 .
There are no comprehensive figures on outcomes of cataract surgery in developing countries and on the relative importance of spectacles, patient selection and surgery. However, at least 25% of the six million cataract operations performed annually in developing countries are believed to have poor outcomes. About one quarter of these are due to surgical complications15 .
Prognosis1 27
Back to contentsAdults
Age-related cataracts are progressive and the progression is variable and unpredictable. Without treatment, most people with a cataract will develop severe visual impairment.
The visual performance of the eye is generally considered in terms of acuity, contrast sensitivity, glare disability, visual fields and colour vision. Outcomes for cataract surgery have mainly been assessed in terms of acuity only.
With surgery, 95% of people will have 6/12 best corrected vision if there is nothing else wrong with the eye.
More recent studies have looked at self-reporting of outcomes and these make it clear that patients may consider surgery unsuccessful in the face of improved visual acuity if, for example, anisometropia or disturbance from the fellow eye results.
One Swedish analysis showed that 84% of patients experienced an overall benefit from surgery, 7% reported no change and 9% reported increased difficulty with activities of daily living18 .
Pre-operative visually significant ocular comorbidity was the most important predictor of poor subjective outcome. Older age was not per se. The greatest benefit was seen for second eye surgery in younger patients.
Patients may be disappointed to find that they require glasses for distant vision after cataract surgery, when they did not require them prior to surgery.
Children
Untreated cataracts in children younger than 10 years of age cause amblyopia, leading to lifelong visual impairment even if the cataracts are later removed.
Most children with a unilateral cataract have normal vision in the eye without the cataract. Most children who have treatment for bilateral cataracts achieve only partial sight.
Driving28
Back to contentsAdvise the patient not to drive and to contact the DVLA if either of the following applies. It is likely to apply where there are severe bilateral cataracts, or after failed bilateral cataract extractions:
Group 1 entitlement (to drive a car or motorcycle)
To read in good daylight (with the aid of glasses or contact lenses if worn) a registration mark fixed to a motor vehicle and containing letters and figures 79 millimetres high and 50 millimetres wide at a distance of 20 metres, or at a distance of 20.5 metres where the characters are 79 millimetres high and 57 millimetres wide.
Visual acuity (with the aid of glasses or contact lenses if needed) must be at least 6/12 with both eyes open (or in the only eye if you have vision in one eye only).
Note that in the presence of cataract, glare may affect your ability to meet the number plate requirements, even if your acuity is good enough.
Group 2 entitlement (to drive a larger vehicle)
To have a visual acuity, using corrective lenses if necessary, of at least 6/7.5 (0.8 decimal) in the better eye and at least 6/12 (0.5 decimal) in the other eye.
The uncorrected acuity in each eye must be at least 3/60.
Where glasses are worn to meet the minimum standards, they should have a corrective power ≤+8 dioptres.
It is also necessary for all drivers of Group 2 vehicles to be able to meet the prescribed and relevant Group 1 visual acuity requirements.
In the presence of a cataract, glare may affect the ability to meet the number plate requirement, even with appropriate acuities.
If there is any uncertainty about fitness to drive, advise the patient to contact the DVLA or to seek clarification from an eye specialist.
Dr Mary Lowth is an author or the original author of this leaflet.
Further reading and references
- Cataracts; NICE CKS, March 2020 (UK access only)
- Allen D, Vasavada A; Cataract and surgery for cataract. BMJ. 2006 Jul 15;333(7559):128-32. doi: 10.1136/bmj.333.7559.128.
- Gupta VB, Rajagopala M, Ravishankar B; Etiopathogenesis of cataract: an appraisal. Indian J Ophthalmol. 2014 Feb;62(2):103-10. doi: 10.4103/0301-4738.121141.
- Haeck IM, Rouwen TJ, Timmer-de Mik L, et al; Topical corticosteroids in atopic dermatitis and the risk of glaucoma and cataracts. J Am Acad Dermatol. 2011 Feb;64(2):275-81. doi: 10.1016/j.jaad.2010.01.035. Epub 2010 Dec 3.
- Tatham A: J Med Case Reports. 2008; 2: 124. Atopic dermatitis, cutaneous steroids and cataracts in children: two case reports
- Braakhuis AJ, Donaldson CI, Lim JC, et al; Nutritional Strategies to Prevent Lens Cataract: Current Status and Future Strategies. Nutrients. 2019 May 27;11(5). pii: nu11051186. doi: 10.3390/nu11051186.
- Zhao L, Chen XJ, Zhu J, et al; Lanosterol reverses protein aggregation in cataracts. Nature. 2015 Jul 30;523(7562):607-11. doi: 10.1038/nature14650. Epub 2015 Jul 22.
- Andley UP; Effects of alpha-crystallin on lens cell function and cataract pathology. Curr Mol Med. 2009 Sep;9(7):887-92.
- Cataracts in adults: management; NICE Guideline (Nov 2017)
- Implantation of multifocal (non-accommodative) intraocular lenses during cataract surgery; NICE Interventional Procedure Guidance, June 2008
- Tabin G, Chen M, Espandar L; Cataract surgery for the developing world. Curr Opin Ophthalmol. 2008 Jan;19(1):55-9.
- Gogate P, Optom JJ, Deshpande S, et al; Meta-analysis to Compare the Safety and Efficacy of Manual Small Incision Cataract Surgery and Phacoemulsification. Middle East Afr J Ophthalmol. 2015 Jul-Sep;22(3):362-9. doi: 10.4103/0974-9233.159763.
- Kamalarajah S, Silvestri G, Sharma N, et al; Surveillance of endophthalmitis following cataract surgery in the UK. Eye. 2004 Jun;18(6):580-7.
- Asbell PA, Dualan I, Mindel J, et al; Age-related cataract. Lancet. 2005 Feb 12-18;365(9459):599-609.
- Yorston D; Cataract complications. Community Eye Health. 2008 Mar;21(65):1-3.
- Moshirfar M, Milner D, Patel BC; Cataract Surgery
- Durand ML; Endophthalmitis. Clin Microbiol Infect. 2013 Mar;19(3):227-34. doi: 10.1111/1469-0691.12118.
- Lundstrom M, Stenevi U, Thorburn W; The Swedish National Cataract Register: A 9-year review. Acta Ophthalmol Scand. 2002 Jun;80(3):248-57.
- Barry P, Seal DV, Gettinby G, et al; ESCRS study of prophylaxis of postoperative endophthalmitis after cataract surgery: Preliminary report of principal results from a European multicenter study. J Cataract Refract Surg. 2006 Mar;32(3):407-10.
- Kaiserman I, Kaiserman N, Elhayany A, et al; Cataract surgery is associated with a higher rate of photodynamic therapy for age-related macular degeneration. Ophthalmology. 2007 Feb;114(2):278-82.
- Welch NR, Gregori N, Zabriskie N, et al; Satisfaction and dysphotopsia in the pseudophakic patient. Can J Ophthalmol. 2010 Apr;45(2):140-3. doi: 10.3129/i09-266.
- Tester R, Pace NL, Samore M, et al; Dysphotopsia in phakic and pseudophakic patients: incidence and relation to intraocular lens type(2). J Cataract Refract Surg. 2000 Jun;26(6):810-6.
- Schwiegerling J; Recent developments in pseudophakic dysphotopsia. Curr Opin Ophthalmol. 2006 Feb;17(1):27-30.
- Davison JA; Positive and negative dysphotopsia in patients with acrylic intraocular lenses. J Cataract Refract Surg. 2000 Sep;26(9):1346-55.
- Makhotkina NY, Berendschot TT, Beckers HJ, et al; Treatment of negative dysphotopsia with supplementary implantation of a sulcus-fixated intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2015 Jun;253(6):973-7. doi: 10.1007/s00417-015-3029-8. Epub 2015 May 7.
- Muhtaseb M, Kalhoro A, Ionides A; A system for preoperative stratification of cataract patients according to risk of intraoperative complications: a prospective analysis of 1441 cases. Br J Ophthalmol. 2004 Oct;88(10):1242-6.
- Nizami AA, Gulani AC; Cataract
- Assessing fitness to drive: guide for medical professionals; Driver and Vehicle Licensing Agency
Continue reading below
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 13 Dec 2026
14 Dec 2021 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free