Examination of the cranial nerves
Peer reviewed by Dr Adrian Bonsall, MBBSLast updated by Dr Colin Tidy, MRCGPLast updated 20 Jun 2014
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
This page has been archived.
It has not been reviewed recently and is not up to date. External links and references may no longer work.
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article:
There are 12 pairs of cranial nerves although the optic nerve is really an extension of the brain rather than a peripheral nerve. The ability to test them swiftly, efficiently and to interpret the findings should be a core competency for general practice. The separate article Neurological History and Examination includes a description of a brief examination of the cranial nerves. Here the aim is to give a slightly fuller account of examination whilst interpretation of the findings is discussed elsewhere in the separate article on Cranial Nerve Lesions.There are also more specific separate articles on Diplopia and III, IV and VI Cranial Nerve Lesions and Visual Field Defects.
Continue reading below
Principles of examination
There is no single way to perform a clinical examination but the following is offered as one effective way. Everyone should develop their own protocol. Protocols are easy to use, efficient in use of time and reduce the chance of missing something significant.
With most examinations, the clinician will detect and interpret the signs. With neurological examination, especially of the sensory system, the doctor relies on the patient to interpret what he/she feels. The patient must be encouraged to report when there is a change in sensation or if anything feels different from normal. Very often there will not be an absence of sensation but a dulling or diminution and this is just as important. Comments such as, 'I can feel it but it's not so sharp over there', are very useful.
By and large, the muscles supplied by the cranial nerves are not as large and powerful as those supplied by spinal nerves, with the exception of those supplied by XI. The following table lists the grading of power for muscles of the limbs and it can be modified accordingly to give a meaningful scale:
MRC scale for muscle power | |
0 | No muscle contraction is visible. |
1 | Muscle contraction is visible but there is no movement of the joint. |
2 | Active joint movement is possible with gravity eliminated. |
3 | Movement can overcome gravity but not resistance from the examiner. |
4 | The muscle group can overcome gravity and move against some resistance from the examiner. |
5 | Full and normal power against resistance. |
It makes sense to examine the nerves in roughly numerical order but there are exceptions where nerves are best grouped together and their numbers may not be sequential.
Olfactory nerve
Most of what we call taste is really smell. Testing the olfactory nerve is often omitted. Before starting, check that there is free flow of air by occluding each nostril in turn and asking the patient to sniff in. The nerves are tested by having bottles containing characteristic substances such as peppermint, coffee or lavender and asking the patient to identify each in turn. If you do not have such tools available, ask the patient to close his/her eyes and then hold a bar of soap under the patient's nose for them to smell.
It is possible to occlude one nostril and then the other to assess each side in turn.
If there is doubt about the claim of anosmia, try testing with ammonia solution. Ammonia causes a physical irritation and so will cause an abreaction even in the presence of anosmia. Denying a response to ammonia suggests malingering.
Continue reading below
Optic nerve
Two important aspects of the optic nerve are visual acuity and visual field.
Visual acuity
Visual acuity can easily be tested with Snellen type. Charts are also available to test ability to read small print. If the patient normally wears spectacles both tests may be done with them on, as it may be assumed that they give good correction and that what is important is any rapid deterioration in visual acuity. Deterioration of at least two lines of the Snellen chart is significant.
Colour vision can be tested with Ishihara plates. Deterioration may be significant but remember that 8% of men and 0.5% of women have congenital X-linked colour blindness.
Visual fields
A small item, such as the top of a pen, may be used to test visual fields by confrontation. Sit about 50 cm away from the patient and ask him/her to keep the eyes fixed on your nose. Hold the point half way between you and move it around, asking the patient to say when it disappears from view. If you also fix on the patient's nose, you can compare the patient's response with yours, taking your own as normal.
Plotting visual field defects by confrontation is very crude and, if an accurate picture is required, it is necessary to ask an optometrist to plot visual fields by perimetry.
Use of the ophthalmoscope
Many people find use of the ophthalmoscope daunting. It can only be mastered with practice and this means using it over the course of years. Do not bother clicking through the lenses until you are adept in its use but use the 0 dioptre lens to view the retina. It is very difficult to see much through a small pupil in a bright room. It should be possible to take the patient to a darker room or to dim the light with curtains or a blind. Better still, a mydriatic agent such as 1% homatropine eye drops can be used, provided that the patient does not have to drive for the rest of the day. The effect can last up to 24 hours.
Take the ophthalmoscope and ask the patient to fix his/her gaze on something in the distance such as a picture on the wall and to ignore you. Do the pupils look equal? First shine the light on the eye and then remove it. The pupil should be brisk in its response of both constriction and dilatation. This is testing both the optic nerve (afferent pathway) and the oculomotor nerve (efferent pathway), as the response is dependent upon appreciation of light and the motor response of the muscles of the iris. There is also a consensual response in that the contralateral pupil will also respond but less markedly.
Then use the ophthalmoscope to examine the eye. First hold it away from the patient and look through it at the eye. There should be an orange reflex from light reflected from the retina. This means that the lens is clear and there is no significant cataract. Check that the optic disc is clear. Note the vessels of the retina and try to see the periphery. Repeat on the other side. It is not reasonable to assume that because one side is normal that the other side will be too.
Only by seeing many normal discs is it possible to be confident about abnormality. Try to learn:
The normal colour of a disc. It is usually pink but in people with dark skin it appears grey. People with blond hair tend to have paler retinae than those with darker hair. Hair may go grey with the passage of time or blond or coloured with the contents of a bottle but the retina is constant.
A clear and distinct optic disc. Only by being familiar with a normal disc is it possible to recognise papilloedema when it occurs. Cupping of the disc, as with glaucoma, brings the vessels up over the disc.
Learn to follow the four arteries and veins. Follow them to the periphery. Note tortuosity. Note any silver wiring or A-V nipping. The appearance of central retinal artery thrombosis and retinal vein thrombosis is described in the respective articles. A detached retina is avascular and may appear as a crescent or a grey cloud.
Only by learning the normal appearance of a retina will such abnormalities as neovascularisation, cotton wool spots and haemorrhages be recognised.
Oculomotor, abducent and trochlear nerves
These three nerves are examined together, as they control the external ocular muscles.
The oculomotor nerve supplies the internal muscles of the eye including sympathetic fibres to dilate the pupil and parasympathetic fibres to constrict it and to reduce the focal length of the lens for accommodation.
Internal ocular muscles
The pupillary response to light has already been tested. It is possible to complement this test by moving a finger from about 40 cm to about 10 cm from the patient's nose, asking him/her to follow it, and noting if the pupil constricts in response to accommodation. This is not normally very marked.
If the pupils are unequal, which eye is the abnormal one?
Darken the room and note if the difference increases. If it does, the problem is due to failure of sympathetic tone to the smaller pupil.
Brighten the room and, if the difference increases, the problem is due to failure of parasympathetic tone to the larger pupil.
If the difference remains constant in dim or bright light, the difference may be physiological.
Failure of sympathetic tone is a feature of Horner's syndrome that is discussed elsewhere. There is lack of sweating on that side of the forehead and possibly a ptosis too. Horner's syndrome is a very good lateralising sign but a poor localising sign.
The Argyll Robertson's pupil is small, does not react to light, but constricts on accommodation. If it is bilateral, the pupils are frequently unequal in size (anisocoria). Argyll Robertson's pupils are almost always related to neurosyphilis but similar pupils are occasionally found in diabetic neuropathy and in some hereditary neuropathies.
The myotonic pupil (Holmes-Adie syndrome) reacts very slowly both to light and accommodation, but especially to light. It may be unilateral or bilateral and occurs more in women than in men. Myotonic pupils may be associated with absence or depression of the tendon reflexes and occasionally with anhidrosis in the limbs.
External ocular muscles
Hold the patient's head still with the left hand and hold out the extended right index finger about 40 cm in front of the patient. Ask the patient to follow your finger with their eyes. Move the finger up and down and left and right. There should be a full range of movements of both eyes. Note any ptosis or lid lag. Then move the finger to the left and hold it there for several seconds whilst the eyes are observed for nystagmus. Repeat to the right. False positive tests for nystagmus can result from holding the finger too close and by moving it too far to the extreme of vision.
It may be apparent that some of the movements are incomplete in one eye. There may also have been a complaint of diplopia. A more sensitive way to test ocular movements is with a small torch. This test is also very useful when assessing children for strabismus and tends to be easier than the 'cover test'.
Hold the torch about 40 cm away and shine it in the patient's eyes. Note the reflection of the light in the centre of the pupil.
Holding the patient's head still, move the torch up, down, left and right, asking them to follow the light with their eyes.
Note if the reflection of the light becomes eccentric from any direction. If so, note in which pupil it was eccentric and the direction of stare.
The lesion is in the muscle that moves that eye in that direction.
External Ocular Paralysis | |||
Muscle | Direction of pull | Result of paralysis | Cranial nerve |
Medial rectus | Medially | Lateral | III |
Superior rectus | Upwards | Downwards | III |
Lateral rectus | Laterally | Medial | VI |
Inferior rectus | Downwards | Upwards | III |
Superior oblique | Down and out | Up and in | IV |
Inferior oblique | Up and out | Down and in | III |
The superior and inferior recti are set slightly medial to the midline. Hence they tend to move the eye slightly medially as well as up or down. This movement is offset by co-ordination with the lateral rectus and oblique muscles.
VI AND XII NERVE PALSIES

Ignore the reflection in the pupils, as the patient is not looking at the light. There is complete failure of the left eye to move laterally, due to paralysis of the lateral rectus muscle supplied by VI nerve.
Continue reading below
Trigeminal nerve
The trigeminal nerve is largely a sensory nerve but it does have a motor component in the mandibular division.
Lightly touch each side of the face with a piece of cotton wool and ask if it feels normal and symmetrical. Alternatively, a light touch with a finger will suffice. Test the areas supplied by the ophthalmic, maxillary and mandibular branches. The spinal nerves from segments C2 and C3 supply the face for about three fingers' breadth in front of the ear.
Ask the patient to clench his/her teeth. Both masseters should feel firm and strong. The contracting temporalis may also be felt. The pterygoids may jut the jaw forwards.
Many neurologists omit the corneal reflex unless a sensory deficit is found, especially in the ophthalmic division, or if there is a lesion of another cranial nerve. Take a clean piece of cotton wool and ask the patient to look away from the side being tested. Gently touch the cornea with the cotton wool and the patient will blink. This requires the sensation of V but also the motor of VII.
There may be a positive jaw jerk reflex in spasticity. This is difficult to elicit and is not described here.
Facial nerve
Ask the patient to give a broad toothy grin, demonstrating what you want. Do not say, 'Show me your teeth', or he/she may remove any dentures and hand them to you. Is the grin full and symmetrical?
Ask the patient to screw up his/her eyes. Gently try to prise them open. You should fail.
Ask the patient to raise his/her eyebrows. Are the furrows of the forehead symmetrical?
Paralysis of the facial nerve causes face drop. This is more marked with a lower motor neurone (LMN) lesion than an upper motor neurone (UMN) lesion. The best way to differentiate between the two is to test the muscles of the forehead. They have bilateral innervation at the upper motor neurone level and so, in a UMN lesion such as a pseudobulbar palsy, they are spared. An LMN lesion such as Bell's palsy will involve the forehead.
Vestibulocochlear nerve
Testing of the vestibular component with such tests as Hallpike's manoeuvre is described in the separate article on Vertigo. Formal testing of the cochlear component requires audiometry. Hearing tests are discussed elsewhere.
Either whispering or use of a high-frequency tuning fork can give a very crude assessment of hearing. A 516 Hz (upper C) tuning fork is usually employed:
Strike the tuning fork and hold it about 2 cm from the ear, asking the patient to tell you when it stops. Then listen to it yourself and the intensity of the sound indicates the degree of loss in that ear.
If it is marked, place the still vibrating fork on the mastoid process and ask if it is heard. If it is heard by bone but not air conduction, there is a marked conductive loss. With profound nerve deafness, the patient may be hearing it by bone conduction in the other ear.
If there is significant loss in one ear, Weber's test can be employed. Strike the tuning fork and place it on the centre of the forehead. Ask the patient in which ear it seems louder. The vibration is conducted through bone and it will be quieter in the bad ear with nerve deafness but louder with conductive deafness as the affected ear becomes more sensitive.
Glossopharyngeal and vagus nerves
Assessment of the glossopharyngeal and vagus nerves is difficult. Ask the patient to swallow. Is there any difficulty? Ask the patient to open his/her mouth wide and to say 'Ahh'. Phonation should be clear and the uvula should not move to one side. The quality of the dysarthria differs for central and peripheral lesions. Central lesions produce a strained, strangled voice quality, while peripheral lesions produce a hoarse, breathy and nasal voice.
It is also possible to test the gag reflex by touching the pharynx with a tongue depressor. Most people omit this unless there is evidence of a local lesion. It is unpleasant and around 20% of normal people have a minimal or absent response.
Isolated lesions of the IX nerve are very rare. Taste to the anterior two thirds of the tongue travels with the VII nerve until it leaves in the chorda tympani to join the V nerve. The posterior third of the tongue is supplied from the IX nerve that also provides parasympathetic fibres to the salivary glands. It is possible to test taste with small bottles and a dropper. The bottles usually contain sugar or salt solution. Most generalists do not perform this test.
Accessory nerve
The accessory nerve supplies the trapezius and sternomastoid muscles. Is there any wasting? Ask the patient to shrug his/her shoulders up and try to push them down. Ask the patient to push his/her head forwards against your hand. Both these movements should be very difficult to resist.
LMN lesions produce weakness of both muscles on the same side. UMN lesions produce ipsilateral sternomastoid weakness and contralateral trapezius weakness, because of differing sources of cerebral innervation.
Hypoglossal nerve
It is often more convenient to assess the XII cranial nerve before the XI as the mouth is examined for IX and X.
Ask the patient to protrude his/her tongue and note any deviation. A fluttering motion called fibrillation rather than fasciculation may be seen with an LMN lesion.
If the tongue deviates to one side when protruded, this suggests a hypoglossal nerve lesion. If it is an LMN lesion, the protruded tongue will deviate towards the side of the lesion. With a UMN lesion, the tongue will deviate away from the side of the lesion.
XII NERVE PALSY
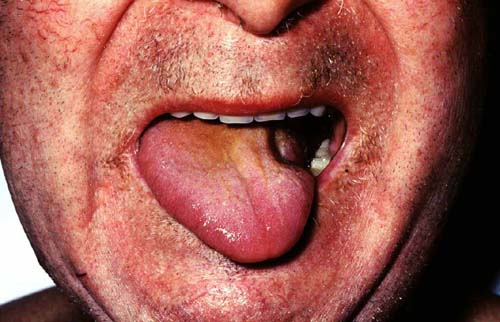
Note the wasted left side of the tongue and deviation to the left suggesting a left LMN lesion.
This article is far from exhaustive and the site below gives further details.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Blumenfeld H; Cranial Nerves, Neuroanatomy through Clinical Cases
Continue reading below
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Adrian Bonsall, MBBS
Medical Author
MA (Chemistry), MBBS (Hons), DCH
Since 2000 Adrian has been employed in emergency and critical care paediatrics based in Sydney, with particular interests in toxicology, trauma and resuscitation.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
20 Jun 2014 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
More in history and examination
- Blurred vision
- Dental and periodontal diseases
- Dyspraxia and apraxia
- Ear, nose and throat examination
- Flatulence and wind
- Gait abnormalities in children
- Gangrene
- Gynaecological examination and history
- Halitosis
- Hearing testing and screening in young children
- Jaundice
- Mother's six-week postnatal check
- Myalgic encephalomyelitis
- Paediatric history
- Palmar erythema
- Proctalgia fugax and anal pain
- Steatohepatitis and steatosis
- Visual field defects
- Voiding difficulties
- Wheezing in children