Corticosteroids and corticosteroid replacement therapy
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 24 May 2023
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Oral steroids article more useful, or one of our other health articles.
In this article:
Continue reading below
History of corticosteroids
Hydrocortisone (cortisol) is secreted by the adrenal cortex and has both glucocorticoid and mineralocorticoid effects. The term 'glucocorticoid' derives from the early discovery that these hormones were important in glucose metabolism.
Since the 1940s synthetic glucocorticoids have been developed for their anti-inflammatory and immunomodulatory effects. Attempts have been made to increase the beneficial effects and reduce the adverse effects by modifying the steroid nucleus and side groups.
Mode of action and relative strengths
A brief outline of complex steroid biosynthesis and physiology is helpful when considering the therapeutic benefits and adverse effects of the glucocorticoids.
The adrenal cortex has three distinct anatomical zones. Glucocorticoids originate from the zona fasiculata (mineralocorticoids from the zona glomerulosa, and androgens from the zona reticularis).
Regulation of glucocorticoid synthesis and release is complex. Glucocorticoids are not stored and must be synthesised when required. The mechanism involves:
The hypothalamo-pituitary axis. Feedback mechanism inhibits production.
Feedback via catecholamines from the adrenal medulla.
The autonomic nervous system.
Glucocorticoids have anti-inflammatory and immunosuppressive effects important in natural immune responses. They are involved in the mobilisation of substrates for gluconeogenesis (amino acids, fatty acids, etc) and maintenance of normal blood glucose by:
Stimulating gluconeogensis in the liver.
Mobilising amino acids from extrahepatic tissues.
Reducing glucose usage by inhibiting uptake in muscle and fat.
Stimulating fat breakdown.
These effects are mediated through the glucocorticoid receptor (GR), an intracellular protein acting as a nuclear transcription factor regulating the expression of a diverse range of genes. This process involving mediation of the main metabolic and cardiovascular effects is called 'transactivation' and the inhibitory effect is called 'transrepression'.
The basal daily rate of cortisol secretion is 6-8 mg per square metre, and this increases tenfold in acute stress. Physiological replacement requires 10-15 mg per square metre because of reduced bioavailability. The different natural and synthetic glucocorticoids have different potencies and pharmacodynamic properties according to:
Relative and absolute affinity for the GR and mineralocorticoid receptor (MR).
Affinity for the associated enzyme.
Ability to modulate the glucocorticoid responsive genes.
The different glucocorticoids also have differing pharmacokinetic properties affecting:
Bioavailability.
Plasma half life.
Clearance rates.
Water solubility, etc.
Steroids compared
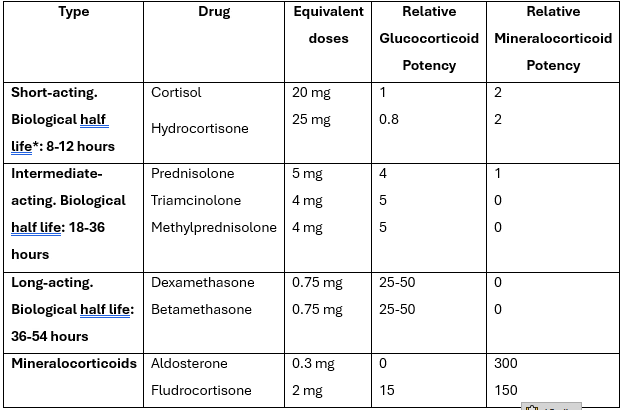
*Duration of adrenocorticotrophic hormone (ACTH) suppression after a single dose of the drug.
Deflazacort is another oral steroid with high glucocorticoid and low mineralocorticoid activity. Deflazacort is derived from prednisolone and deflazacort 6 mg is equivalent to prednisolone 5 mg.
Continue reading below
Indications and benefits of corticosteroids
Corticosteroids can be life-saving and have dramatic benefits. However, their therapeutic use has to be balanced against the risks of serious adverse effects.
Dose, route of administration, duration of treatment and choice of corticosteroid must be considered to maximise therapeutic benefit and minimise adverse effects.
The list of conditions below clearly illustrates the diverse range of benefits that are possible.
Conditions where corticosteroids have been used with evidence-based benefits include : | |
Giant cell arteritis (temporal arteritis). | Minimal change glomerulonephritis. Acute leukaemia. Idiopathic thrombocytopenic purpura. Cerebral oedema. Congenital adrenal hyperplasia. Anaphylaxis and allergic reactions. |
Drug initiation and choice of steroid
Benefits should be weighed against risks.
Every patient should be given a steroid card. Patients should also be given the manufacturer's patient information leaflet with their prescription.
Steroids are commonly used at high initial dose and then reduced to maintain remission.
The choice of steroid is made according to properties required. For example:
Hydrocortisone and cortisone have glucocorticoid effects but relatively high mineralocorticoid activity. They are therefore unsuitable for long-term use, but useful intravenously (IV) in emergency situations. Hydrocortisone can be used topically with less risk of side-effects as it is less potent.
Prednisolone has high glucocorticoid activity with less mineralocorticoid effect and is used for longer-term treatment.
Betamethasone and dexamethasone have even higher glucocorticoid activity and insignificant mineralocorticoid effect. They can thus be used when high dosages are required without effects such as fluid retention - for example, cerebral oedema from malignancy. They cross the placenta readily and should be avoided in pregnancy.
Long duration of action with betamethasone and dexamethasone makes them useful in conditions like congenital adrenal hyperplasia when suppression of corticotrophin must be maintained.
Local treatments should be used when possible in preference to systemic.
Adrenal suppression can be reduced by:
Morning dosage.
Alternate day dosing.
Intermittent courses of treatment.
Addition of small doses of immunosuppressive drug.
STEROID TREATMENT CARD
I am a patient on steroid treatment which must not be stopped suddenly.
Notes for patients:
If you have been taking this medicine for more than three weeks, the dose should be reduced gradually when you stop taking steroids unless your doctor says otherwise.
Read the patient information leaflet given with the medicine.
Always carry this card with you and show it to anyone who treats you. For one year after you stop treatment you must mention that you have taken steroids.
If you become ill, or if you come into contact with anyone who has an infectious disease, consult your doctor promptly. If you have never had chickenpox, you should avoid close contact with people who have chickenpox or shingles. If you do come into contact with chickenpox, see your doctor urgently.
Make sure the information on the card is kept up-to-date.
Continue reading below
Disadvantages of corticosteroids
Adverse effects are dose-related and often predictable according to the glucocorticoid actions (eg, diabetes, osteoporosis, muscle wasting, neuropsychiatric effects) and mineralocorticoid actions (eg, hypertension, and electrolyte and fluid balance).
There is a wide range of adverse effects:
Cardiovascular: hypertension; congestive cardiac failure.
Central nervous system: mood disturbance (including mania), psychosis, sleep disturbance.
Endocrine/metabolic: adrenal suppression, growth failure in children, insulin resistance, diabetes, disturbance of thyroid function, hypokalaemia, metabolic alkalosis.
Gastrointestinal: gastric effects (peptic ulceration, etc), fatty liver.
Haematopoietic: leucocytosis and other effects (eg, reduced eosinophils and monocytes).
Immune system:
Suppression type IV hypersensitivity (interferes with Mantoux test).
Inhibitory effects (leucocytes, macrophages, cytokines).
Suppression of primary antigen response (important with vaccines).
Musculoskeletal system:
Myopathy (especially proximal muscles).
Avascular necrosis of bone.
Ophthalmic: cataracts (more common in children), elevation of intraocular pressure, glaucoma.
Skin and other systems: moon face, truncal obesity, dorsolumbar hump, acne, thin skin, skin striae (violaceous), impotence, irregular periods.
Scenarios
In addition to the disadvantages of longer-term treatment, there are several clinical scenarios worthy of special mention:
Corticosteroids and surgery
Adrenal suppression caused by steroid therapy may result in an inadequate adrenocortical response to surgery (acute adrenocortical insufficiency can precipitate hypotension and death). Therefore:
Anaesthetists must be informed when patients have taken corticosteroids within three months of surgery (10 mg or more) so that:
For minor surgery under general anaesthesia either the usual corticosteroid dose can be given orally, or 25-50 mg of hydrocortisone can be given IV at induction.
For moderate/major surgery the usual oral dose is taken on the day of surgery with hydrocortisone as above at induction and the same IV dose three times daily for between 24 and 72 hours after surgery, depending on the extent of surgery. This is then followed by the usual oral dose.
Patients on prolonged treatment with potent inhaled or nasal corticosteroids should have the same precautions taken as above before surgery.
Corticosteroids and live vaccines
Live vaccines should not be given within three months of:
An adult receiving 40 mg/day of prednisolone or equivalent for more than a week.
A child receiving either 2 mg/kg/day for one week or 1 mg/kg/day for one month.
Corticosteroids in pregnancy and breastfeeding1
Corticosteroids vary in their ability to cross the placenta. Prednisolone is mostly inactivated as it crosses the placenta, whereas betamethasone and dexamethasone cross readily.
Although corticosteroids can cause abnormalities in fetal development in animals, this has not been shown in humans (for example, cleft lip and palate).
Prolonged or repeated corticosteroid administration in pregnancy increases the risk of intrauterine growth restriction (IUGR). Short-term treatment carries no such risk.
The theoretical risk of adrenal suppression in neonates after prenatal exposure to corticosteroids is not clinically important and resolves spontaneously after birth.
Prednisolone is excreted in small amounts in breast milk and is unlikely to cause systemic effects in the infant unless doses exceed 40 mg daily. Above this dose, infants should be monitored for adrenal suppression. No data are available on other corticosteroids.
Corticosteroids and infection
Corticosteroids affect the severity and clinical presentation of infections as well as susceptibility to infections. For example:
Ocular infections may be exacerbated (fungal and viral).
Diagnosis of serious infection may be delayed (septicaemia, tuberculosis).
Corticosteroids may activate or exacerbate infections (tuberculosis, amoebiasis, strongyloides).
Corticosteroids predispose to fungal infections in chronic lung disease (pulmonary aspergillosis).2 3
Topical corticosteroids probably predispose to eczema herpeticum, although the association may not be as strong as is often suggested.4
Patients on corticosteroids should avoid exposure to measles and seek medical advice if exposed. Prophylaxis with human normal immunoglobulin may be given.1
Corticosteroids and chickenpox
Patients on corticosteroids (systemic but not topical, rectal or inhaled) or who have used them within three months and are non-immune to varicella infection, are at risk of severe chickenpox. Infection can be severe (fulminant pneumonia, hepatitis and disseminated intravascular coagulation, often without prominent rash). Therefore:
Exposed non-immune patients on or within three months of taking corticosteroids should be given passive immunisation with varicella-zoster immunoglobulin (within three days, and no later than 10 days, after exposure).
Confirmed chickenpox in such patients warrants urgent referral and urgent treatment.1
Corticosteroids and osteoporosis
Corticosteroid therapy is a major risk factor for osteoporosis.5 See also the separate article on Osteoporosis Risk Assessment and Primary Prevention.
Steroids and the skin
Systemic and local side-effects can occur, particularly with moderate-strength steroids. The emphasis should be on appropriate use to produce benefit and to minimise side-effects. Once-daily applications are recommended by the National Institute for Health and Care Excellence (NICE).6 Information on use of steroids in dermatology can be found in the separate article Topical Steroids for the Skin. Important areas for consideration include:
Appropriate strength of steroids.
Use of emollients with steroids.
Clear instructions for patients.
Regular follow-up.
Inhaled and nasal corticosteroids1
Systemic absorption may follow nasal administration, particularly if high doses are used or if treatment is prolonged.
High doses of inhaled corticosteroids used for prolonged periods can induce adrenal suppression. Inhaled corticosteroids have been associated with adrenal crisis and coma in children. Excessive doses should be avoided.
Drug interactions
Important interactions include:7
Antagonism of antihypertensives.
Exacerbation of gastrointestinal side-effects (eg, non-steroidal anti-inflammatory drugs (NSAIDS) and peptic ulcer).
Enhanced anticoagulant effects.
Antagonism of diabetic drugs.
Exacerbation of hypokalaemia with digoxin, diuretics, theophyllines and beta2 agonists.
Impaired immune response of vaccines.
Monitoring and stopping steroids
Monitoring must include regular monitoring for side effects of oral steroids and to ensure that the appropriate dose of oral steroid is being prescribed, as well as monitoring of the disease being treated.
In patients whose disease is unlikely to relapse, steroids should be reduced gradually when they have:1
Received more than 40 mg prednisolone (or equivalent) daily for more than one week.
Been given repeat doses in the evening.
Received more than three weeks' treatment.
Recently received repeated courses (particularly if taken for longer than three weeks).
Taken a short course within one year of stopping long-term therapy.
Other possible causes of adrenal suppression.
The dose may be reduced rapidly to physiological doses of about 7.5 mg of prednisolone and then more slowly, at the same time ensuring that disease relapse does not occur.
Patients not in the groups above (eg, who have received fewer than three weeks of corticosteroids) can usually have corticosteroids stopped abruptly.
Further reading and references
- Hodgens A, Sharman T; Corticosteroids.
- British National Formulary (BNF); NICE Evidence Services (UK access only)
- Bille J, Marchetti O, Calandra T; Changing face of health-care associated fungal infections.; Curr Opin Infect Dis. 2005 Aug;18(4):314-9.
- Brakhage AA; Systemic fungal infections caused by Aspergillus species: epidemiology, infection process and virulence determinants. Curr Drug Targets. 2005 Dec;6(8):875-86.
- Wollenberg A, Zoch C, Wetzel S, et al; Predisposing factors and clinical features of eczema herpeticum: a retrospective analysis of 100 cases.; J Am Acad Dermatol. 2003 Aug;49(2):198-205.
- Osteoporosis - prevention of fragility fractures; NICE CKS, April 2023 (UK access only)
- Frequency of application of topical corticosteroids for atopic eczema; NICE Technology appraisal guidance, August 2004
- Corticosteroids - oral; NICE CKS, June 2020 (UK access only)
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 10 May 2028
24 May 2023 | Latest version

Feeling unwell?
Assess your symptoms online for free