Cricothyroidotomy
Peer reviewed by Dr Adrian Bonsall, MBBSLast updated by Dr Gurvinder Rull, MBBSLast updated 15 Oct 2014
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
This page has been archived.
It has not been reviewed recently and is not up to date. External links and references may no longer work.
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article:
Synonym: cricothyrotomy
This procedure provides a temporary emergency airway in situations where there is obstruction at or above the level of the larynx, such that oral/nasal endotracheal intubation is impossible. Compared with an emergency tracheostomy, it is quicker and easier to perform and associated with fewer complications.1It is a relatively quick procedure, taking up to about two minutes to complete.2In an emergency, without access to medical equipment, cricothyroidotomy has even been improvised using a drinking straw and penknife.3
There are three techniques:
Needle.
Intubation (with purpose-built kits).
Surgical.
All require a good working knowledge of regional anatomy to be able to carry the procedure out safely and effectively. It should be used as a last resort, reserved for life-and-death situations and is best carried out by experienced hands, or under their instruction where possible. The techniques can be taught on animal or mannequin models.4However, conditions in the 'field' are frequently much more challenging.
Continue reading below
Indications2
Need for an emergency airway where:
Intubation is not possible via the oral or nasal route.
Severe maxillofacial trauma.
Oedema of throat tissues preventing visualisation of the cords (eg, angioneurotic oedema, anaphylaxis, burns, smoke inhalation).
Severe oropharyngeal/tracheobronchial haemorrhage.
Foreign body in upper airway.
Lack of equipment for endotracheal intubation.
Technical failure of intubation.
Severe trismus/clenched teeth.
Masseter spasm after succinylcholine.
Contra-indications2
Back to contentsAvailability of a less invasive means of securing the airway.
Patients <12 years old (needle technique may be used but formal tracheostomy is preferred).
Laryngeal fracture.
Pre-existing or acute laryngeal pathology.
Tracheal transection with retraction of the trachea into the mediastinum.
Anatomical landmarks obscured by gross haemorrhage/surgical emphysema, etc.
Continue reading below
Technique5
Back to contentsNeedle cricothyroidotomy
A needle or cannula (usually a large-bore IV cannula) is inserted through the cricothyroid membrane:
Place the patient supine and, assuming there is no cervical spine injury, extend the neck using a pillow under the shoulders.
Run a finger down the front of the neck in midline and find the notch in the upper border of the thyroid cartilage. Below this is a depression between the thyroid and cricoid cartilages - the cricothyroid membrane.
CRICOTHYROIDOTOMY (1)
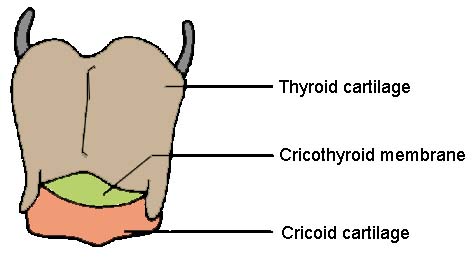
Stabilise the cricothyroid membrane with one hand between finger and thumb.
Pierce it with a large-bore cannula (14 G) attached to a syringe aiming at 45° to the skin, caudally in the sagittal plain.
Aspirate as the needle is introduced and confirm position by withdrawal of air; slide the cannula over the needle into the airway.
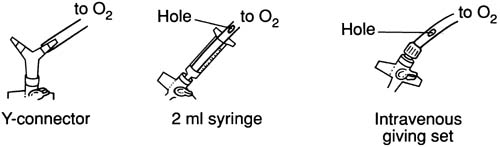
Connect to an O2 supply via Y-connector - give 15 L/minute for an adult or, in a child, set the gas flow to the age of the child in years.
Ventilate by covering the patent port of Y-connector with a thumb to allow O2 to flow for one second (transtracheal insufflation). Remove thumb to allow expiration for four seconds via the upper airway. If no Y-connector is available, use a 2 ml syringe or IV giving set with a hole in the side that can be occluded by the thumb.
CRICOTHYROIDOTOMY (2)
NB: expiration is not possible through the cannula so with complete upper airway obstruction of the upper airway, reduce the oxygen flow. A needle cricothyroidotomy can usually only be used for 30-45 minutes before CO2 retention becomes significant.
Cricothyroid intubation with purpose-built kits
Cricothyroidotomy may be achieved with a narrow tube using a pre-prepared kit such as the Mini-Trach® II which contains a guarded blade, plastic introducer, 4 mm uncuffed tube to slide over introducer, ISO connection, tracheal suction tube and neck fastenings. The patient can breathe spontaneously or be bagged using this form of airway, but they are usually only used as a temporary measure until a more permanent airway is secured. Retrograde intubation can be practised with a Mini-Trach® II set by passing the introducer upwards into the mouth and feeding an endotracheal tube into place over it.6
Surgical cricothyroidotomy
This is usually not performed in children aged under 12.
Delineate anatomy as above, clean the skin and instil a local anaesthetic (if the patient is conscious).
Make a small vertical skin incision in the midline, spread the wound edges laterally and identify the cricothyroid membrane.
Take care not to cut or remove the thyroid or cricoid cartilages.
Make a horizontal incision through the membrane's inferior half and then extend gently through it.
Dilate the opening with curved forceps or rotation of an inverted scalpel handle. Insert a small, cuffed endotracheal tube or tracheotomy tube (maximum 8 mm).
Aim downwards as the tube is inserted to avoid damage to the vocal cords.
Inflate the tube cuff and confirm its position with visualisation of chest movements and auscultation over the lungs and stomach.
Finally, secure the tube.
Complications
Back to contentsAlthough complications do occur, they are minor when compared with the catastrophic outcome normally associated with a failure to secure an airway. Complications can affect up to 40% in the emergency situation but, in experienced hands, the complication rate is usually much lower. Elective complication rate is ~ 6-8%.2
|
|
Thyrohyoid membrane incision | Attention to anatomy; vertical skin incision; confirm position of the cricothyroid membrane after skin incision. |
Intraoperative/postoperative bleeding | Incise directly over the cricothyroid membrane in the midline; vertical skin incision; horizontal incision in inferior half membrane; avoid the thyroid isthmus. |
Subglottic stenosis | Use a small-bore tube; avoid long-term use (>72 hours). |
Dysphonia/hoarseness | Use a small tube; point inferiorly to avoid cords; avoid tracheal cartilage damage by not using force. |
Laryngeal damage | Avoid oversized tube and excessive traction on the thyroid cartilage during insertion. |
Tube misplaced in bronchus | Avoid insertion of too much of tube length so as not to enter the right main bronchus. |
Pulmonary aspiration | Protect the upper airway by suction and positioning. |
Tracheal stenosis | Use a low-pressure balloon cuff. |
Recurrent laryngeal nerve injury | Stay in midline and avoid the posterior subglottic wall by not inserting instruments too far. |
Oesophageal perforation or tracheo-oesophageal fistula | Do not incise or insert the needle deeply after entering the subglottic space. |
Tracheo-left brachiocephalic vein fistula | Use a low-pressure cuff. |
Fracture of thyroid cartilage | Avoid an oversized tube. |
Continue reading below
Prognosis
Back to contentsAs cricothyroidotomy is usually performed as an emergency airway procedure of last resort, patients receiving them tend to be critically ill. Unsurprisingly, one study from the USA showed that only 27% of trauma patients receiving pre-hospital cricothyroidotomy survived to hospital discharge but 62% survived to emergency department admission, indicating reasonable utility as a holding emergency airway.7Amongst longer-term survivors, good functional status is unusual, with frequent neurological disability.8
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Varaday SS, Yentis SM, Clarke S; A homemade model for training in cricothyrotomy. Anaesthesia. 2004 Oct;59(10):1012-5.
- Ellis H; Applied anatomy of cricothyrotomy and tracheostomy. Br J Hosp Med (Lond). 2006 Sep;67(9):M168-9.
- Hsiao J, Pacheco-Fowler V; Videos in clinical medicine. Cricothyroidotomy. N Engl J Med. 2008 May 29;358(22):e25.
- Gerich TG, Schmidt U, Hubrich V, et al; Prehospital airway management in the acutely injured patient: the role of surgical cricothyrotomy revisited. J Trauma. 1998 Aug;45(2):312-4.
- Boon JM, Abrahams PH, Meiring JH, et al; Cricothyroidotomy: a clinical anatomy review. Clin Anat. 2004 Sep;17(6):478-86.
- Adams BD, Whitlock WL; Bystander cricothyroidotomy performed with an improvised airway. Mil Med. 2002 Jan;167(1):76-8.
- Wong DT, Prabhu AJ, Coloma M, et al; What is the minimum training required for successful cricothyroidotomy?: a study in mannequins. Anesthesiology. 2003 Feb;98(2):349-53.
- Advanced Paediatric Life Support, 4th Edition. Advanced Life Support Group. BMJ Books 2005
- Slots P, Vegger PB, Bettger H, et al; Retrograde intubation with a Mini-Trach II kit. Acta Anaesthesiol Scand. 2003 Mar;47(3):274-7.
- Fortune JB, Judkins DG, Scanzaroli D, et al; Efficacy of prehospital surgical cricothyrotomy in trauma patients. J Trauma. 1997 May;42(5):832-6; discussion 837-8.
- Isaacs JH Jr; Emergency cricothyrotomy: long-term results. Am Surg. 2001 Apr;67(4):346-9; discussion 349-50.
Continue reading below
About the authorView full bio

Dr Gurvinder Rull, MBBS
Medical Author, Consultant: Clinical Pharmacology, Therapeutics and General Internal Medicine
BSC (Hons), MBBS, FRCP, MA (Medical Ethics)
Dr Gurvinder Rull qualified in 2000, joining EMIS’s content authoring team (now Patient.info) in 2007.
About the reviewerView full bio

Dr Adrian Bonsall, MBBS
Medical Author
MA (Chemistry), MBBS (Hons), DCH
Since 2000 Adrian has been employed in emergency and critical care paediatrics based in Sydney, with particular interests in toxicology, trauma and resuscitation.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
15 Oct 2014 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free