Baker's cyst
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Philippa Vincent, MRCGPLast updated 16 Mar 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
A Baker's cyst is a swelling that can develop behind the knee. It is filled with the lubricating fluid that is usually found inside the knee joint, known as "synovial fluid". It most commonly occurs if there is an underlying problem with the knee such as osteoarthritis. Symptoms can include pain, swelling and tightness behind the knee. Sometimes, a Baker's cyst can split open (rupture) and cause symptoms in the calf that can be similar to a deep vein thrombosis (DVT). A Baker's cyst often gets better and disappears by itself over time. However, there are various treatments that may help if there are symptoms associated with it.
At a glance
A Baker's cyst is a fluid-filled swelling behind the knee, also called a popliteal cyst.
It can develop when there is an underlying knee problem, such as arthritis or a meniscal tear.
Some people have no symptoms, but larger cysts can cause visible swelling, aching, or tightness.
The cyst often gets better by itself over time, but it can persist for months or years.
Treatment aims to relieve symptoms and address any underlying knee issues.
Occasionally, a cyst may rupture, causing fluid to leak into the calf.
What is a Baker's cyst?
A Baker's cyst is a fluid-filled swelling that can develop behind the knee. It is one cause of knee pain.
It is named after a doctor called William Baker who first described this condition in 1877. It is also sometimes called a popliteal cyst, as the medical term for the area behind the knee is the popliteal fossa.
The cyst can vary in size fromvery small to large (it can be several centimetres across). Rarely, a Baker's cyst can develop behind both knees at the same time.
Understanding the knee joint
The first side-view diagram below illustrates a typical normal knee joint looking from the side.
Baker's cyst diagram
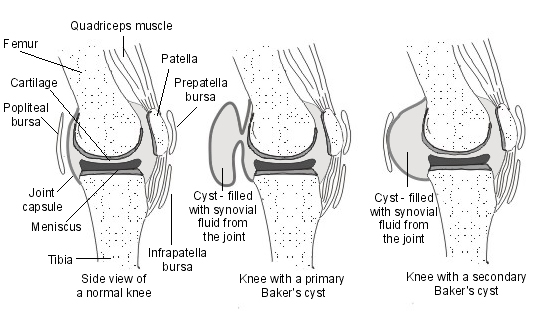
The joint capsule is a thick structure that surrounds the whole knee and gives it some support. It is lined by a special membrane called the synovium. The synovium produces a fluid called synovial fluid. This fluid acts as a lubricant within the knee joint and helps to cushion it during movement.
There are also various tissue pouches called bursae next to the knee. A bursa is a small sac of synovial fluid with a thin lining. Bursae are normally found around joints and in places where ligaments and tendons pass over bones. They help to reduce friction and allow maximal range of motion around joints. The bursa at the back of the knee is called the popliteal bursa.
Each knee joint also contains a medial and a lateral meniscus. These are thick rubber-like pads of cartilage tissue. The menisci cartilage sit on top of, and are in addition to, the usual thin layer of cartilage which covers the top of one of the bones of the lower leg, called the tibia. They act as shock absorbers to absorb the impact of the upper leg on the lower leg. They also help to improve smooth movement and stability of the knee.
What causes a Baker's cyst?
There are two ways in which a Baker's cyst may form.
A primary Baker's cyst
A Baker's cyst may develop just behind an otherwise healthy knee joint. This type of cyst is sometimes referred to as a primary or idiopathic Baker's cyst and usually develops in younger people and in children.
It is thought that, in this type of Baker's cyst, there is a connection between the knee joint and the popliteal bursa behind the knee. This means that synovial fluid from inside the joint can pass into the popliteal bursa and a Baker's cyst can form.
A secondary Baker's cyst
It is more common for a Baker's cyst to develop if there is an underlying problem within the knee, such as arthritis or a tear in the meniscal cartilage that lines the inside of the knee joint. T This is sometimes referred to as a secondary Baker's cyst.
In a secondary Baker's cyst, the underlying problem within the knee joint causes too much synovial fluid to be produced within the joint. As a result of this, the pressure inside the knee increases and this has the effect of stretching the joint capsule. The joint capsule bulges out into the back of the knee, forming the Baker's cyst that is filled with synovial fluid.
How common is a Baker's cyst?
Baker's cysts are most common between the ages of 35 and 70, particularly if there is an underlying knee condition. As above, primary Baker's cysts can occur in children, typically between the ages of 4 and 7.
Arthritis is the most common condition associated with Baker's cysts. This can include various different types of arthritis, such as osteoarthritis (most common), rheumatoid arthritis, psoriatic arthritis and gout.
Baker's cysts may also develop if you have had a tear to the meniscus or to one of the ligaments within the knee, or if you have had an infection within your knee joint.
Baker's cyst symptoms
Some people with a Baker's cyst do not have any symptoms at all. Small cysts may not always be found during a knee examination and thehe cyst may be found incidentally wduring an investigation on the knee, such as a scan.
Usually, larger Baker's cysts are more likely to cause symptoms. The swelling behind the knee might be able to be seen or felt;. . some people feel an ache around the knee area. It may be difficult to bend the knee if there is a large Baker's cyst and the area behind the knee may feel tight, especially when standing up. Less commonly, there may be a sensation of clicking or locking of theknee.
If there is an underlying knee problem such as arthritis, there may also be symptoms related to that, such as knee pain or swelling of the knee joint itself.
Complications
The most common complication of a Baker's cyst is for it to split open (rupture) - this is thought to happen in about 1 in 20 Baker's cysts. If this happens, the fluid from inside the cyst can leak out into the calf muscle and cause swelling of the calf. Sometimes redness and itching of the skin of the calf can develop as a result of irritation caused by this fluid.
If a Baker's cyst ruptures, it can sometimes be difficult to tell the difference between the ruptured cyst and a deep vein thrombosis (DVT). A DVT is a blood clot that forms in a leg vein. In these cases, it is important that investigations are carried out to exclude a DVT because it can be a serious condition that needs treatment. See the separate leaflet called Deep Vein Thrombosis for more detail.
Very rarely, a Baker's cyst may become infected.
How is a Baker's cyst diagnosed?
A Baker's cyst is usually diagnosed by an examination of the kneeThe swelling feels as though it is fluid filled and it might be "transilluminable" (a light can be seen through it) which confirms the diagnosis of a cyst.
Usually no investigations are needed to confirm the diagnosis. If there is a doubt about the diagnosis then an ultrasound scan (or occasionally an MRI scan) might be used. If there is a concern about a DVT then specific tests (usually a Doppler ultrasound scan) will be arranged in hospital.
Baker's cyst treatment
A Baker's cyst usually gets better and disappears by itself over time. However, the cyst may persist for months or even years before it goes. Most people have very few symptoms and no specific treatment is needed.
There are various treatment options that may help if there are symptoms associated with a Baker's cyst. These include:
Treatment of any underlying knee problem
It is important that any underlying knee problem is treated. This may help to reduce the size of a Baker's cyst and any swelling or pain that it causes. For example, if there is osteoarthritis of the knee joint, a steroid injection into the knee may help to relieve pain and inflammation. However, this does not always stop the cyst from coming back again.
If there is an injury to the knee such as a meniscal tear, treatment of this may help to treat the Baker's cyst as well. See the separate leaflets called Knee Ligament Injuries and Meniscal Tears (Knee Cartilage Injuries) for more detail.
Treatment to help relieve symptoms
If the Baker's cyst is causing pain or discomfort, one or more of the following may be helpful:
Non-steroidal anti-inflammatory drugs (NSAIDs). These can help to relieve pain and may also limit inflammation and swelling. There are many types and brands. Some - such as ibuprofen or naproxen - can be bought over the counter from a pharmacy. Others require a prescription. NSAIDs can cause side-effects - inflammation of the lining of the stomach which can cause pain and bleeding is the most serious. Regular or long-term use can cause damage to the kidneys and it is important to have regular blood tests if taking this medication regularly. Some people with asthma, high blood pressure, kidney failure and heart failure may not be able to take NSAIDs so it is important to check with the pharmacist before buying these.
Stronger pain relief. If the cyst ruptures, the fluid from inside the cyst may leak into the calf and cause worse pain. In this situation, stronger medication may be needed on prescription.
Ice may also help to reduce swelling and pain. An ice pack can be made by wrapping ice cubes in a plastic bag or towel and applying it to the area for 10-30 minutes. (Ice should never be put directly next to the skin as it may cause ice-burn.) A bag of frozen peas is an alternative.
Crutches. Very occasionally, crutches may be needed to help to take the weight off the affected leg whilst walking for a few days until the symptoms ease.
Physiotherapy. Keeping the knee joint moving and using strengthening exercises to help the muscles around the knee is often very helpful.
Other treatments
There are some other treatment options that are sometimes used:
Fluid drainage - sometimes a doctor may use a needle to drain excess fluid from the knee joint to help to relieve the symptoms. However, it is common for the Baker's cyst to re-form over time.
Cortisone (steroid) injection - this is sometimes used following fluid drainage, to reduce the pain and inflammation caused by the cyst. It does not prevent it from coming back again.
Surgery to remove the cyst - this is sometimes done, especially if a cyst is very large or painful and/or other treatments have not worked. Sometimes a keyhole method is used to close off the connection between the Baker's cyst and the knee joint. The cyst is also sometimes removed using open surgery. Surgery may be carried out to treat an underlying problem at the same time - for example, repairing a meniscal tear.
Patient picks for Knee pain

Bones, joints and muscles
Chondromalacia patellae
Chondromalacia patellae is damage to the cartilage at the back of the kneecap (patella). The usual treatment advised is to avoid overuse of the knee and to have physiotherapy, which is effective in most cases.
by Dr Philippa Vincent, MRCGP

Bones, joints and muscles
Housemaid's knee
Housemaid's knee is also known as prepatellar bursitis. It is caused by inflammation of a small fluid-filled sac (the bursa) in front of the kneecap. It more commonly occurs in people who spend long periods of time kneeling. Treatment is usually supportive and the outlook is generally very good.
by Dr Colin Tidy, MRCGP
Frequently asked questions
Can I have a Baker's cyst in both knees at the same time?
Yes, although it's rare, a Baker's cyst can sometimes develop behind both knees simultaneously.
When is a Baker's cyst most likely to occur?
Baker's cysts are most common in adults between the ages of 35 and 70, particularly if there is an existing knee problem. Primary Baker's cysts can also occur in children, typically between 4 and 7 years old.
What should I do if a Baker's cyst ruptures?
If a Baker's cyst ruptures, the fluid can leak into the calf muscle, causing swelling, and sometimes redness and itching. It's important to get this checked, as the symptoms can be similar to a deep vein thrombosis (DVT), which is a serious condition that needs urgent medical attention.
How is a Baker's cyst usually diagnosed?
A Baker's cyst is typically diagnosed through a physical examination of the knee. The swelling usually feels fluid-filled, and a doctor might check if light can be seen through it. Usually, no further investigations are needed for confirmation, though an ultrasound or MRI might be used if there's doubt about the diagnosis or concern about a DVT.
How long does a Baker's cyst typically last?
A Baker's cyst often gets better and disappears on its own over time, but it can persist for months or even years before fully resolving.
Further reading and references
- Herman AM, Marzo JM; Popliteal cysts: a current review. Orthopedics. 2014 Aug;37(8):e678-84. doi: 10.3928/01477447-20140728-52.
- Frush TJ, Noyes FR; Baker's Cyst: Diagnostic and Surgical Considerations. Sports Health. 2015 Jul;7(4):359-65. doi: 10.1177/1941738113520130.
- Zhou XN, Li B, Wang JS, et al; Surgical treatment of popliteal cyst: a systematic review and meta-analysis. J Orthop Surg Res. 2016 Feb 15;11:22. doi: 10.1186/s13018-016-0356-3.
- Abate M, Di Carlo L, Di Iorio A, et al; Baker's Cyst with Knee Osteoarthritis: Clinical and Therapeutic Implications. Med Princ Pract. 2021;30(6):585-591. doi: 10.1159/000518792. Epub 2021 Aug 2.
About the authorView full bio

Dr Philippa Vincent, MRCGP
General Practitioner, Medical Author
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent is an NHS GP working in North London.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 14 Mar 2028
16 Mar 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in bones, joints and muscles
- Ankle injury
- Axial spondyloarthritis
- Back and spine pain
- Cauda equina syndrome
- Cervical rib
- Chondromalacia patellae
- Fibromyalgia
- Gout
- Hand-arm vibration syndrome
- Hip fracture
- Knee ligament injuries
- Multiple sclerosis
- Osteoarthritis
- Polymyalgia rheumatica
- Rotator cuff injuries and disorders
- Shoulder pain
- Sports injuries
- Tennis elbow
- Torticollis
- Whiplash neck sprain