Deep vein thrombosis
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Toni Hazell, FRCGPLast updated 15 Sept 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:How to prevent DVT when travelling
A deep vein thrombosis (DVT) is a blood clot in a vein. Blood clots in veins most often occur in the legs but can occur elsewhere in the body, including the arms. This leaflet is about blood clots in leg veins.
The most common cause of a blood clot developing in a vein is immobility. A complication can occur in some cases where part of the blood clot breaks off and travels to the lung (pulmonary embolus). This is usually prevented if you are given anticoagulation treatment.
At a glance
A deep vein thrombosis (DVT) is a blood clot that develops in one of your deep veins, usually in the leg.
Common symptoms include pain, tenderness, and swelling of the calf, which may also become warm and red.
The most common cause of a DVT is immobility, especially during or after surgery.
A DVT can lead to a pulmonary embolus (PE) if part of the clot travels to the lungs.
Treatment includes anticoagulant medicines, compression stockings, resting with legs raised, and keeping active.
Regular movement, especially during long journeys or after surgery, helps prevent DVTs.
What is a deep vein thrombosis?
What is deep vein thrombosis?
A deep vein thrombosis (DVT) is a blood clot that develops in one of your deep veins. It usually occurs in your leg and makes that leg become very painful and swollen. The clot may travel up to your lungs to cause a pulmonary embolus.
Diagram of leg showing veins and a Deep Vein Thrombosis
Deep leg veins are the larger veins that go through the muscles of the calf and thighs. They are not the veins that you can see just below the skin; neither are they the same as varicose veins. When you have a DVT, the blood flow in the vein is partially or completely blocked by the blood clot.
A calf vein is the common site for a DVT. A thigh vein is less commonly affected. Rarely, other deep veins in the body can be blocked by blood clots.
A DVT is part of a group of problems together known as venous thromboembolism.
Causes of a deep vein thrombosis
Blood normally flows quickly through veins and does not usually become solid (clot). Blood flow in leg veins is helped along by leg movements, because muscle action squeezes the veins. Sometimes a DVT occurs for no apparent reason. However, the following increase your risk of having a DVT:
Immobility which causes blood flow in the veins to be slow. Slow-flowing blood is more likely to clot than normal-flowing blood and those who are admitted to hospital should be assessed for their DVT risk soon after admission, and preventative measures put in place if needed.
A surgical operation where you are asleep (under general anaesthetic) is the most common cause of a DVT. Your legs are still when you are under anaesthetic, because the muscles in your body are temporarily paralysed. Blood flow in the leg veins can become very slow, making a clot more likely to occur. Certain types of surgery (particularly operations on the pelvis or legs) increase the risk of DVT even more.
Any illness or injury that causes immobility increases the risk of DVT. This includes having a leg in a hard plaster cast after a fracture. People who are admitted to intensive care units are at an increased risk of DVT. This is due to a number of reasons but partly because they are very ill and also because they are immobile (they may even be kept asleep by anaesthetic medications). Those being discharged from hospital with a problem that affects movement of the legs should also have a risk assessment and treatment if appropriate.
Long journeys by plane, train or coach/car may cause a slightly increased risk. This is because you are mostly sitting for long periods of time and not moving around very much.
Damage to the inside lining of the vein increases the risk of a blood clot forming. For example, a DVT may damage the lining of the vein. So, if you have a DVT then you have an increased risk of having another one in the future. Some conditions, such as inflammation of the vein wall (vasculitis) and some medicines (for example, some chemotherapy medicines), can damage the vein and increase the risk of having a DVT. Damage to the vein can also happen with injury to the vein caused by a needle. This might occur after treatment with a drip in hospital (where a tube is inserted into a vein to get fluids into you). Drug users who inject drugs, such as heroin, can also damage their veins, making DVTs more common. This is especially the case if they inject illegal drugs into their leg or groin.
Conditions that cause the blood to clot more easily than normal (thrombophilia) can increase the risk. Some conditions can cause the blood to clot more easily than usual. Examples include nephrotic syndrome and antiphospholipid syndrome. See the separate leaflets called Nephrotic Syndrome, Antiphospholipid Syndrome and Thrombophilia for more details. Some rare inherited conditions can also cause the blood to clot more easily than normal. An example of an inherited blood disorder which can cause DVTs is factor V Leiden mutation. You are more at risk of a DVT if you have a family history of DVTs - that is, a close relative who has had one.
Contraceptive pills, patches and rings and hormone replacement therapy (HRT) which contain oestrogen can cause the blood to clot slightly more easily. Women taking the combined oral contraceptive (COC) pill or tablet HRT have a small increased risk of DVT. HRT which is transdermal (given through the skin as a patch, gel or spray) does not carry an increased risk of DVT, and nor does vaginal oestrogen given as part of HRT.
People with cancer or heart failure have an increased risk. Sometimes a DVT happens in a person who has not yet been diagnosed with cancer. Investigations looking for the cause of a DVT may show cancer to be the underlying cause.
Older people (over 60 years of age) are more likely to have a DVT, particularly if they have poor mobility or have a serious illness such as cancer.
Pregnancy increases the risk. About 1 in 1,000 pregnant women have a DVT while they are pregnant, or within about six months after they give birth.
Obesity and being overweight also increases the risk. If your body mass index (BMI) is more than 25 kg/m2, you are more at risk of DVT.
Lack of fluid in the body (dehydration) can make a DVT more likely to happen. Effectively, the blood becomes stickier and more liable to clot.
How common is a deep vein thrombosis?
It is estimated that about 1 in 1,000 people have a DVT each year in the UK.
Deep vein thrombosis symptoms
A DVT most commonly develops in a deep vein below the knee in the calf. Typical DVT symptoms include:
Pain and tenderness of the calf.
Swelling of the calf.
Colour and temperature changes of the calf. Blood that would normally go through the blocked vein is diverted to outer veins. The calf may then become warm and red.
Sometimes there are no symptoms and a DVT is only diagnosed if a complication occurs, such as a pulmonary embolus (PE) - see below.
Diagnosing a deep vein thrombosis
Sometimes it is difficult for a doctor to be sure of the diagnosis from just your symptoms, as there are other causes of a painful and swollen calf. Examples of conditions that can cause similar symptoms are muscle strains or skin infections (cellulitis).
Your doctor might calculate something called a Wells' score to work out the likelihood of you having a DVT. It involves looking at your symptoms and risk factors for a DVT. The doctor will also consider whether there are any symptoms or signs to suggest that the clot has travelled to your lungs and caused a PE.
If you have a suspected DVT, you will normally be advised to have tests done urgently to confirm or rule out the diagnosis. Two commonly used tests are:
D-dimer blood test
This detects fragments of breakdown products of a blood clot. The higher the level, the more likely you are to have a blood clot in a vein. Unfortunately, the test can be positive in a number of other situations, such as if you have had recent surgery or if you are pregnant.
A positive test does not, therefore, diagnose a DVT. The test may, however, indicate how likely it is that you have a blood clot (the clot can be either a DVT or a PE) and can help decide if further tests are needed.
Duplex Doppler
This special type of ultrasound is used to show blood flow in the leg veins and any blockage to blood flow. Ultrasound is useful because it is an easy, non-invasive test. Ideally this test should be done within four hours - this often isn't practically possible, in which case an injection of blood-thinning medicine (anticoagulant) may be given while you are waiting for the scan.
Other tests
Sometimes these tests are not conclusive and more detailed tests are necessary. Contrast venography is another test that can be done. In this test a dye is injected into the leg veins.
X-ray tests can then detect the dye which is shown not to be flowing if a vein is blocked by a clot. Computerised tomography (CT) scans and magnetic resonance imaging (MRI) scans are also very occasionally needed.
Complications of a deep vein thrombosis
When a blood clot forms in a leg vein it usually remains stuck to the vein wall. The symptoms tend to settle gradually. However, there are two main possible complications of DVT:
A blood clot that breaks off and travels to the lung (pulmonary embolus).
Persistent calf symptoms (post-thrombotic syndrome).
Pulmonary embolus (PE)
In a small number of people who have a DVT, a part of the blood clot breaks off. This travels in the bloodstream and is called an embolus. An embolus will travel in the bloodstream until it becomes stuck. An embolus that comes from a clot in a leg vein will be carried up the larger leg and body veins to the heart, through the large heart chambers, but will get stuck in a blood vessel going to a lung. This is called a pulmonary embolus.
DVTs and PEs are known collectively as venous thromboembolism
A small PE may not cause any symptoms. A medium-sized PE can cause breathing problems and chest pain. A large PE can cause collapse and sudden death. It is estimated that if people with DVT are not treated, about half of them would develop a PE large enough to cause symptoms or death.
Post-thrombotic syndrome
Without treatment, up to 5 in 10 people who have a DVT develop long-term symptoms in the calf. This is called post-thrombotic syndrome. Symptoms occur because the increased flow and pressure of the diverted blood into other veins can affect the tissues of the calf.
Symptoms can range from mild to severe and include calf pain, discomfort, swelling and rashes. An ulcer on the skin of the calf may develop in severe cases.
Post-thrombotic syndrome is more likely to occur if the DVT occurs in a thigh vein or extends up into a thigh vein from a calf vein. It is also more common in people who are overweight or obese, in those who are older, and in those who have had more than one DVT in the same leg.
Aims of treatment for a deep vein thrombosis
The aims of treatment are:
To prevent the clot spreading up the vein and getting larger. This may prevent a large embolus breaking off and travelling to the lungs (a PE).
To reduce the risk of post-thrombotic syndrome developing.
To reduce the risk of venous ulcers in the leg in future. This can happen to people who have developed post-thrombotic syndrome.
To reduce the risk of a further DVT in the future.
Deep vein thrombosis treatment
Anticoagulation - preventing the clot from becoming larger
Anticoagulation is often called thinning the blood. Medicines which work in this way are called anticoagulants. However, they do not actually thin the blood. They alter certain chemicals in the blood to stop clots forming so easily. Anticoagulants do not dissolve the clot.
Anticoagulation prevents a DVT from getting larger and prevents any new clots from forming. The body's own healing mechanisms can then get to work to break up the clot.
If you have a DVT, you will usually need an anticoagulant medicine for at least three months and you should then have a specialist review. There are a number of options:
Warfarin has been the usual anticoagulant for many years. The aim is to get the dose of warfarin just right so the blood will not clot easily, but not too much, which may cause bleeding problems. You will need regular blood tests (called INRs) whilst you take warfarin. The INR (which stands for International Normalised Ratio) is a blood test that measures your blood clotting ability. You need the tests quite often at first but then less frequently once the correct dose is found. An INR of 2.5 is the aim if you have warfarin for a DVT, although anywhere in the range 2-3 is OK. If you have had recurrent DVTs, or have had a PE whilst on warfarin, you might need a higher INR (even 'thinner' blood). Recently, some alternatives to warfarin have become available, which do not need regular blood tests.
Rivaroxaban, apixaban, edoxabanand dabigatran are newer anticoagulant medicines. You do not have to have regular blood tests to monitor your blood clotting. This is an advantage over warfarin. However, there is no antidote (as there is with warfarin) to stop you bleeding too easily. These newer tablets are not suitable for everybody.
NICE recommends:
Apixaban or rivaroxaban for confirmed DVT or PE.
If neither apixaban nor rivaroxaban is suitable, then either:
Low molecular weight heparin (LMWH) injections for at least 5 days followed by dabigatran or edoxaban, or
LMWH injections with Warfarin for at least 5 days, followed by Warfarin on its own.
A serious embolus is rare if you start anticoagulation treatment early after a DVT.
If you are pregnant, regular heparin injections rather than anticoagulant tablets may be used. This is because anticoagulant medicines can potentially cause harm (birth defects) to the unborn child.
The length of time you will be advised to take anticoagulation depends on various factors. If you have a DVT during pregnancy or after an operation, then after the birth, or when you are fit again, the increased risk is much reduced. So, anticoagulation may be only for a few months. On the other hand, some people continue to have an increased risk of having a DVT. In this case, the anticoagulation may be long-term.
As a guide, for a DVT that happens below the knee, you will need at least six weeks of anticoagulant treatment. You will need at least three months of treatment if the DVT is above the knee. Some people at higher risk of another DVT may need longer than this. The length of time of anticoagulation varies from person to person. Your doctor or anticoagulant clinic will advise you how long your treatment will be for.
Compression stockings
Some people who develop a DVT are advised to wear compression stockings. Compression stockings are also known as compression hosiery or thromboembolic deterrent stockings ('TEDs'). These are used only to treat ongoing symptoms - they used to be recommended to reduce the risk of getting another DVT, or to reduce the risk of post-thrombotic syndrome, but this is no longer recommended.
The stockings work by applying pressure from outside the veins. This helps squeeze the blood in the veins back up the legs. This then makes the pressure inside the veins less. In turn this prevents leakage of blood into the surrounding tissues.
Before compression stockings are advised you may need to have a test to check that the circulation through the arteries of your legs is normal. This is usually done by a nurse, with a handheld machine called a Doppler. This measures the pressure in your arteries.
Compression stockings come in light, medium or strong material (class 1, 2 or 3) and are worn below the knee. Most people can tolerate class 2. If class 2 is too uncomfortable or difficult, class 1 is prescribed. If class 2 stockings do not work it may be necessary to try class 3, although many people find these difficult to wear for any length of time.
These can be prescribed by your doctor, and obtained at the chemist.
Further tips on support stockings
They are available in different colours, so do ask for the one that suits you best. That way, you are more likely to use them.
They should be removed at bedtime and put on first thing in the morning. It is important to put them on before your legs start to swell in the mornings.
There are open or closed toe options. Open toe stockings may be useful if:
You have painful toes due to arthritis or infection.
You have large feet.
You want to wear socks over your support stockings.
You prefer them.
Stockings should be replaced every 3-6 months. Each time you should be measured again, just in case the size needs to be changed.
You should always have at least two pairs prescribed so that one pair can be washed and dried while the other is worn.
Do not tumble dry support stockings, as this may damage the elastic.
They can be made to measure if none of the standard sizes fit you. This can still be done with a prescription.
Support stocking applicator aids are available if you are unable to get them on. You can discuss this with your pharmacist or nurse.
Walking regularly but raising your leg whilst resting
Unless your doctor advises against this, you should walk regularly after you are discharged from hospital. Walking is thought to improve circulation in the affected leg and may help to reduce your risk of further DVT.
When you are resting, as much as possible - raise your leg. This reduces the pressure in the calf veins and helps to prevent blood and fluid from pooling in the calves. Raised means that your foot is higher than your hip so gravity helps with blood flow returning from the calf. The easiest way to raise your leg is to recline on a sofa with your leg up on a cushion. Sitting on the sofa or in a chair, with your feet on a footstool or pouffe, is not keeping your feet up - the feet are well below your hips in this position.
Raise the foot of the bed a few inches if it is comfortable to sleep like this. This is so your foot and calf are slightly higher than your hip when you are asleep.
Other treatments
Sometimes other treatments may be considered - for example:
Clot-busting (thrombolytic) therapy with medicines such as streptokinase or urokinase. These may help to dissolve a blood clot. The medicine is given directly into the vein and sometimes directly to the clot by a tube (catheter). Studies report this treatment results in fewer people developing post-thrombotic syndrome. It is not yet known if it makes people less likely to have a PE, or another DVT.
Sometimes an operation (called an embolectomy) is done to remove a blood clot from the leg vein or pulmonary artery. These operations are not routine and it is not clear if they are an effective treatment in most cases.
Occasionally, an operation is done to place a filter in the large vein above the blocked leg vein. The aim is to stop any blood clots from travelling up to the lungs. This may be considered if anticoagulation cannot be given (for various reasons), or if anticoagulation fails to prevent clots breaking off and travelling up into the larger veins and up to the lungs.
Preventing a first, or recurrence of, deep vein thrombosis
A DVT is often just a one-off event after a major operation.
However, some people who develop a DVT have an ongoing risk of a further DVT - for example, if you have a blood clotting problem, or continued immobility. As mentioned above, you may be advised to take anticoagulation medicine long-term. Your doctor will advise you about this.
Other things that may help to prevent a first or recurrent DVT include the following:
If possible, avoid long periods of immobility, such as sitting in a chair for many hours. If you are able to, get up and walk around now and then. A daily brisk walk for 30-60 minutes is even better if you can do this. The aim is to stop the blood pooling and to get the circulation in the legs moving. Regular exercise of the calf muscles also helps. You can do some calf exercises even when you are sitting.
Major operations are a risk for a DVT - particularly operations to the hip, lower tummy (abdomen) and leg. There are a number of methods to help reduce this risk:
To help prevent a DVT, you may be given an anticoagulant such as a heparin injection just before an operation. This is called prophylaxis. Enoxaparin and dalteparin are the most common types of heparin given for prophylaxis against blood clots. The new medicine, fondaparinux sodium, can also be given by injection in some circumstances to prevent DVT in surgical patients or immobile medical patients in hospital.
The newer anticoagulant medicines discussed above can be used to prevent DVT or PE after hip or knee replacement surgery. Rivaroxaban, apixaban and dabigatran are used in these situations, and can be given by mouth as a tablet, rather than injection.
An inflatable sleeve connected to a pump to compress the legs during a long operation may also be used.
You may also be given compression stockings to wear whilst you are in hospital.
It is now common practice to get you up and walking as soon as possible after an operation.
When you travel on long plane, train, car or coach journeys, you should have little walks up and down the aisle every now and then. Try to exercise your calf muscles whilst sitting in your seat. (You can do this by circling your ankles, getting into a 'tiptoe' position and lifting your toes off the floor whilst keeping your heels on the ground.) You should aim to stay well-hydrated and avoid alcohol and sleeping medications. See the separate leaflet called Preventing DVT When You Travel for more details. If you have had a previous DVT, you should see a private travel clinic doctor, or your hospital consultant if you are still under their care, for advice before you travel on a long journey or fly. Your GP is unlikely to be trained or insured to give you this advice.
People who are overweight or obese have an increased risk of DVT. Therefore, to reduce your risk, you should try to lose weight.
Reducing the risk of having a DVT in hospital
There has been increased awareness of patients in hospital being at risk of a DVT. This has led to National Institute for Health and Care Excellence (NICE) recommendations on reducing the risk of having a DVT in hospital - see Further Reading below. The purpose of the guideline is to protect people in hospital from blood clots by making sure that:
Everyone has their risk of blood clots checked when they are admitted to hospital (including mental health units), whatever type of treatment they are having.
Each person's risk check is used to decide whether they need treatment to prevent clots - for example, blood-thinning medicines, compression stockings or foot pumps.
If people need blood-thinning medicines to stop clots, they have their risk of bleeding checked first.
Staff explain how important it is for people to stick to their treatments after leaving hospital, because a blood clot can develop weeks later.
In summary
The main cause of DVT is immobility - especially during or after surgery.
If you are having major surgery, you will usually be given medication with injections and/or tablets, to prevent blood clots forming. This is called thromboprophylaxis.
The most serious complication of DVT is a PE, where part of the blood clot breaks off and travels to the lung. PEs can cause death.
Persistent calf symptoms may occur after a DVT.
With treatment, the risk of the above two complications is much reduced.
Treatment includes anticoagulation medicines, compression stockings, leg elevation when sitting, and keeping active.
Prevention is important if you have an increased risk of DVT - for example, during long operations or when you travel on long journeys.
Patient picks for Blood vessel disorders

Heart health and blood vessels
Coronary artery spasm
Coronary artery spasm is a temporary, sudden narrowing of one or more of the coronary arteries.
by Dr Hayley Willacy, FRCGP
Heart health and blood vessels
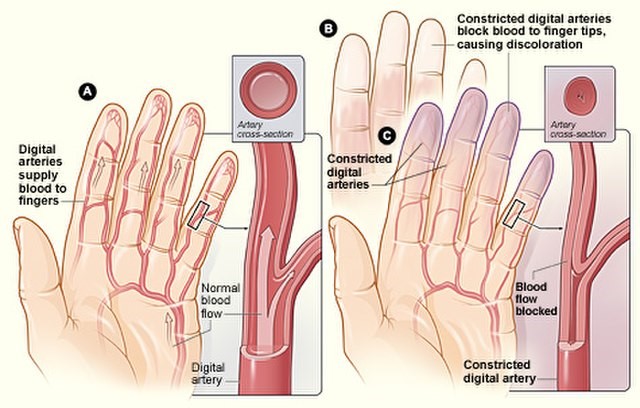
Raynaud's phenomenon
Raynaud's phenomenon (often just called Raynaud's), is a condition where the small blood vessels of the fingers become narrow (constrict). This happens most often when they are in a cool environment. Blood vessels to other extremities such as the toes, ears and nose may also be affected. It is named after Dr Maurice Raynaud, the man who first described it in 1862.
by Dr Hayley Willacy, FRCGP
Frequently asked questions
Can varicose veins cause DVT?
No, varicose veins are a different type of vein problem and are not the same as the deep veins where a DVT forms. Deep leg veins are the larger veins that go through the muscles of the calf and thighs, not the veins you can see just below the skin or varicose veins.
How long does it take for a DVT to dissolve?
Anticoagulant medicines do not dissolve the clot themselves. They work by preventing the DVT from getting larger and stopping new clots from forming. The body's own healing mechanisms then work to break up the existing clot over time.
How to sleep with a DVT in the leg?
When resting, it is advised to raise your leg so that your foot is higher than your hip. This helps gravity assist with blood flow returning from the calf and reduces pressure in the calf veins. You can raise the foot of your bed a few inches if it's comfortable, so your foot and calf are slightly higher than your hip while you sleep.
What can dislodge a DVT?
A part of a deep vein blood clot can break off and travel in the bloodstream. This is called an embolus. This embolus can then travel to the lungs, causing a pulmonary embolus.
What do blood clots look like?
The article describes the symptoms of a DVT in the leg, which include pain, tenderness, and swelling of the calf. The affected calf may also become warm and red. However, the appearance of the clot itself is not described as it is internal.
Further reading and references
- Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism; NICE Guideline (March 2018 - updated August 2019)
- Venous thromboembolic diseases: diagnosis, management and thrombophilia testing; NICE Guidance (March 2020 - last updated August 2023)
- Venous thromboembolism in adults; NICE Quality standard, August 2021
- Compression stockings; NICE CKS, May 2022 (UK access only)
- Deep vein thrombosis; NICE CKS, June 2023 (UK access only)
- Broderick C, Watson L, Armon MP; Thrombolytic strategies versus standard anticoagulation for acute deep vein thrombosis of the lower limb. Cochrane Database Syst Rev. 2021 Jan 19;1(1):CD002783. doi: 10.1002/14651858.CD002783.pub5.
About the authorView full bio

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 13 Sept 2028
15 Sept 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in heart health and blood vessels
- Abdominal aortic aneurysm
- Acute coronary syndrome
- Beta-blockers
- Bradycardia
- Coronary angiography
- Dilated cardiomyopathy
- Electrocardiogram
- Familial hypercholesterolaemia
- Granulomatosis with polyangiitis
- High blood pressure
- Living with high blood pressure
- Low blood pressure
- Mitral stenosis
- Myocardial perfusion scan
- Osler-Weber-Rendu syndrome
- Peripheral arterial disease
- Pulmonary oedema
- Superficial thrombophlebitis
- Thiazide diuretics
- Venous leg ulcers