Coronary angioplasty
Peer reviewed by Dr Toni Hazell, FRCGPLast updated by Dr Doug McKechnie, MRCGPLast updated 9 Nov 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Coronary angioplasty is a treatment to widen narrowed sections of the heart (coronary) arteries. It is also known as percutaneous coronary intervention (PCI). It involves the use of a thin, flexible tube (called a catheter) which is inserted into coronary arteries, via an artery in the wrist or groin and eventually the large blood vessels. It was developed as an alternative to major heart surgery, and is now the first-choice treatment for most people with heart attacks.
The small balloon at the tip of the catheter is blown up at the narrowed section of artery to open it up. A small mesh tube (called a stent) is usually left in place to keep the artery widened.
At a glance
A coronary angioplasty opens blocked or narrowed heart arteries to improve blood flow.
It can be an emergency treatment for a heart attack or a planned procedure for angina.
During the procedure, a balloon is inflated inside the artery, usually leaving a stent.
Mild chest pain may occur during the balloon inflation.
There are risks, but serious complications are uncommon, affecting fewer than 1 in 100 people.
Recovery involves avoiding heavy activity and not driving for a week after the procedure.
Taking prescribed anti-clotting medicines after the procedure is very important.
What is a coronary angioplasty used for?
Coronary angioplasty is used:
In an emergency, to treat people who are having a heart attack (myocardial infarction), or have recently had one. Coronary angioplasty is used to open up blocked arteries that have caused the heart attack, allowing blood to flow to the affected area of the heart and reducing heart damage. Coronary angioplasty (and stent placement) can be life-saving for people with a heart attack.
As a planned ('elective') procedure, for people with angina. Coronary angioplasty can be used to open up narrowed arteries. It can help symptoms of angina. Now, it's usually only offered if medicines haven't been successful at controlling anginal symptoms.
How is a coronary angioplasty performed?
You lie on a couch in a catheterisation room. An X-ray machine is mounted above the couch. Your heart rate, blood pressure, oxygen levels and heart rhythm will be monitored during the entire procedure. A thin, flexible 'guide' tube (catheter) is inserted through a wide needle or small cut in the skin into a blood vessel in the groin or wrist.
Local anaesthetic is injected into the skin above the blood vessel. So, it should not hurt when the catheter is passed into the blood vessel. The doctor gently pushes the catheter up the blood vessel towards the heart.
Low-dose X-rays are used to monitor the progress of the catheter tip which is gently manipulated into the correct position. You may be able to see the progress of the catheter on the X-ray monitor.
Once the catheter has reached the coronary arteries, dye is injected through the catheter. This dye shows up on the X-ray images, filling the coronary arteries and showing any narrowing or blockages. This part of the procedure is called an 'angiogram'.
Once the narrowing is identified, the tip of the catheter is pushed down through the coronary artery down to where there is a narrowed section caused by the fatty patches, or 'plaques', (atheroma). A second thinner 'balloon catheter' is then passed down the 'guide' catheter.
There is a balloon and a small tube (a stent) at the tip of the balloon catheter. The balloon is inflated for 30-60 seconds. This squashes the atheroma and widens the narrowed artery. When the balloon is blown up it stops the blood flow. Therefore, you may have an angina-like chest pain for a short time. However, this soon goes after the balloon is deflated.
Usually, a stent is left in the widened section. The stent is like a wire mesh tube which gives support to the artery and helps to keep the artery widened. The 'collapsed' stent covers the balloon and is opened as the balloon is blown up.
Some stents are coated with a chemical that helps to prevent the artery from becoming blocked again. People who are known to have an allergy to nickel may need a nickel-free stent.
The procedure may be repeated for one or more other narrowed sections within the coronary arteries.
Sometimes, if the narrowing (plaque) is very hard, or too tight for the balloon to get through, a procedure called 'rotablation' may be needed. Rotablation involves passing a catheter (tube) with a tiny drill on its tip over the guide wire, which gradually chips away at the plaque to open it up. This isn't painful, but can cause some mild chest discomfort.
You cannot feel the catheter inside the blood vessels. You may feel an occasional missed or extra heartbeat during the procedure. This is normal and of little concern. During the procedure your heartbeat is monitored by electrodes placed on your chest which provide a tracing on an electrocardiograph (ECG) machine. Sometimes a sedative is given before the test if you are anxious.
Coronary angioplasty
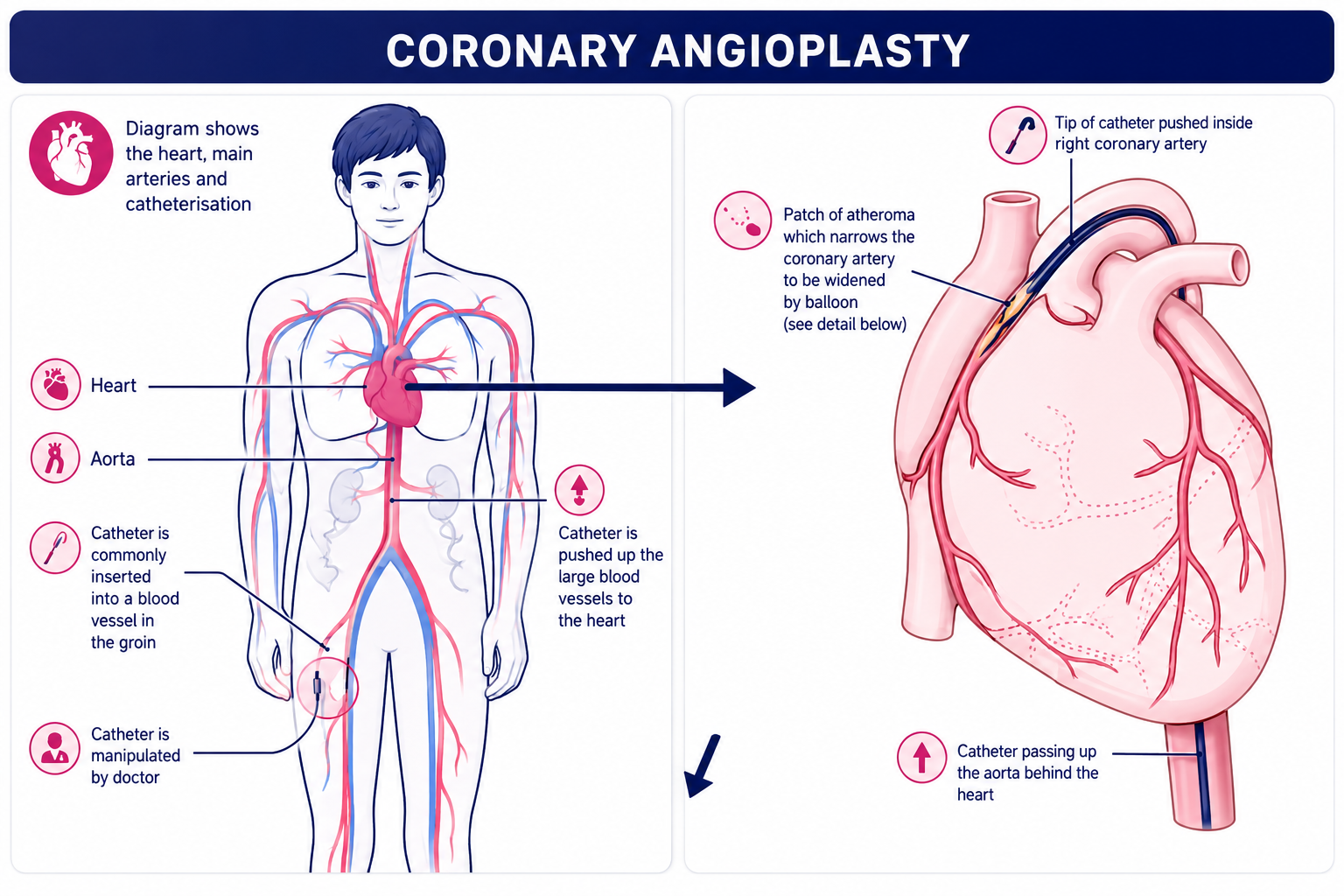
This image shows the path through the blood vessels that the angioplasty catheter uses to get to the coronary arteries.
Angioplasty and stent
This image shows how an angioplasty and stent placement is performed.
How safe is a coronary angioplasty?
A coronary angioplasty is a commonly-used procedure, and is a safer alternative to heart surgery for treating blockages in the coronary arteries.
Coronary angioplasties do, though, have risks. How likely these risks are to happen differs from person to person, and is linked to things such as their age and any other medical conditions that they have. In general, though, serious complications are relatively uncommon, happening in fewer than 1 in 100 angioplasties.
See "Complications of a coronary angioplasty" below.
How to prepare for a coronary angioplasty
You should receive instructions from your local hospital about what you need to do. The sort of instructions may include:
If you take 'blood-thinning' medicines such as warfarin or another anticoagulant, you may need to stop this for 2-3 days before the test (to prevent excessive bleeding from the site of the thin, flexible tube (catheter) insertion). Always tell your hospital team if you are taking a blood-thinning medicine, and take their advice about when to stop and restart them.
If you take insulin or medicines for diabetes, you may need to alter the timing of when you take these. Some medicines may need to be stopped for 48 hours. Your doctor should clarify this with you.
You may be asked to stop eating and drinking for a few hours before the procedure.
You may be asked to shave both groins before the procedure.
You will have to sign a consent form at some point before the test to confirm that you understand the procedure, understand the possible complications (see below) and agree to the procedure being done.
How long does a coronary angioplasty take?
If just one section of artery is widened, the procedure usually takes about 30 minutes. If several sections are to be widened then the procedure takes longer. You may need to stay in hospital overnight for observation following the procedure.
Recovering from a coronary angioplasty
After a coronary angioplasty, you should avoid heavy activities, such as lifting, for a week or until the small wound where the catheter was inserted is healed.
Driving
You shouldn't drive a car or a motorcycle for one week after having an angioplasty.
If you've had a heart attack, and had an unsuccessful angioplasty, you shouldn't drive for four weeks.
If you have a bus, coach, or lorry licence, you must inform the DVLA. You shouldn't drive for at least 6 weeks after the angioplasty, and will need a medical assessment before you can start driving again. The DVLA may ask for further tests to check that you meet the medical standard for driving.
Work
How long it takes to return to work depends on your job, especially how physically strenuous it is.
In general:
After an elective (planned) angioplasty, most people can return to work after a week.
After an emergency angioplasty (to treat a heart attack), it may take several weeks or months before you are well enough to return to work.
Speak to your doctor for advice on your individual situation.
Sex
Avoid having sex until the puncture site (in the wrist or groin) has healed - at least several days.
After that, you can start having sex again when you feel ready to do so. Sex is equivalent to mild-to-moderate physical exercise (for example, climbing two flights of stairs). So, when you are able to do that without feeling short of breath, having chest pain, or feeling very tired, you should be able to have sex again.
After having an elective angioplasty, you might feel ready to have sex again after a few days.
After an angioplasty for a heart attack, it might take longer before you're ready - usually at least two to four weeks.
Complications of a coronary angioplasty
Coronary angioplasties are generally safe procedures, but there are risks. Serious complications are relatively uncommon, usually occurring in fewer than 1 in 100 people. How likely they are differ from person to person and on the situation; for example, complications may be more likely if the angioplasty is treating a complicated artery blockage.
Risks and complications of a coronary angioplasty during, or shortly after, the procedure include:
Bruising around the puncture site (wrist or groin). This is common and usually settles after a few days.
A large pooling of blood under the skin near to the puncture site, caused by damage to the artery wall (pseudoaneurysm). This is uncommon.
Failure of the procedure. Sometimes, it's not possible to stretch the blocked or narrowed arteries. This might mean that a coronary artery bypass graft - a type of open heart surgery - is required instead.
Infection at the puncture site (wrist or groin).
An allergic reaction to the contrast dye.
Kidney damage due to the contrast dye (uncommon, and usually reversible, but more of a risk in people who already have kidney problems).
Serious damage to a coronary artery, requiring emergency heart surgery to fix. This is rare.
A heart attack caused by the procedure. This is uncommon.
A stroke caused by the procedure. This is uncommon.
Rarely, serious complications of the procedure can cause death.
Longer-term risks of coronary angioplasty include:
The treated coronary artery narrowing again (restenosis) over time. This is less likely with newer stents and medicines. If it does occur, it may be treatable with another angioplasty.
A blood clot forming in the stent, causing a blockage of the artery and a heart attack. This is rare, but can be very serious. Medicines such as aspirin and clopidogrel, prasugrel, or ticagrelor are prescribed after an angioplasty to prevent blood clots from forming in the stent. It's very important to take these as prescribed.
How successful is a coronary angioplasty?
Coronary angioplasty and stent placement is a very effective treatment for heart attacks. It has mostly replaced treatment with clot-busting drugs, as it's more effective. It's successful in opening the blocked coronary artery in around 9 out of 10 cases, and can be life-saving. For large heart attacks, coronary angioplasty is best done as soon as possible to reduce damage to the heart muscle.
For people with stable angina, coronary angioplasty can improve symptoms of angina. It improves symptoms of angina quicker than medicines alone. However, in stable angina, coronary angioplasty doesn't prevent future heart attacks, and doesn't make you live any longer. By contrast, medicines for angina do reduce the risk of having a heart attack, and can also control angina symptoms. So, cardiologists often advise treating angina with medications, and keeping the option of an angioplasty in reserve in case symptoms aren't well-controlled enough by medicines.
Sometimes, the narrowing of the coronary arteries can be too complex to treat with angioplasty; for example, the narrowing might be too long, too tight, or there might be too many. If this is the case, coronary artery bypass surgery may be required. However, angioplasty techniques are becoming more and more sophisticated over time, and have become better at treating complex narrowings.
Patient picks for General treatments

Treatment and medication
TENS machines
For some people with certain types of pain, a transcutaneous electrical nerve stimulation (TENS) machine is used as an alternative to painkilling medication.
by Dr Hayley Willacy, FRCGP

Treatment and medication
Probiotics and prebiotics
Probiotics are microscopic, live organisms (microbes) that, if you swallow in large enough amounts, are good for your gut health. Prebiotics are foods that help to increase the numbers and activity of healthy microbes in your gut.
by Dr Colin Tidy, MRCGP
Frequently asked questions
What is rotablation and why is it sometimes used during an angioplasty?
Rotablation is a procedure that may be needed if the narrowing in a coronary artery is very hard or too tight for a balloon to pass through. It involves using a catheter with a tiny drill on its tip, which gradually chips away at the plaque to open up the artery. This procedure is not painful, but it can cause some mild chest discomfort.
How long do I need to stay in the hospital after a coronary angioplasty?
If only one section of an artery is widened, the procedure usually takes about 30 minutes. You may need to stay in the hospital overnight for observation after the procedure, but in many cases, if it's a planned procedure, you might be discharged on the same day.
What kind of activities should I avoid after an angioplasty and for how long?
After a coronary angioplasty, you should avoid heavy activities, such as lifting, for about a week or until the small wound where the catheter was inserted has healed. It's important to allow the puncture site time to recover properly.
Can I drive after having a coronary angioplasty?
You should not drive a car or a motorcycle for one week after an angioplasty. If you had an unsuccessful angioplasty after a heart attack, you should not drive for four weeks. If you have a bus, coach, or lorry licence, you must inform the DVLA and will need a medical assessment before driving again, with at least a six-week waiting period.
What is a stent and why is it used?
A stent is a small, wire mesh tube that is usually left in the widened section of the artery after the balloon is inflated. Its purpose is to provide support to the artery and help keep it widened, preventing it from narrowing again. Some stents are coated with a chemical to further reduce the risk of re-blocking.
What is a pseudoaneurysm and how common is it?
A pseudoaneurysm is a large pooling of blood under the skin near the puncture site, caused by damage to the artery wall. It is an uncommon complication following a coronary angioplasty.
What happens if the angioplasty procedure is not successful in clearing the blockage?
Sometimes it's not possible to stretch the blocked or narrowed arteries effectively with an angioplasty. In such cases, a coronary artery bypass graft, which is a type of open heart surgery, might be required instead. However, angioplasty techniques are continuously improving.
Further reading and references
- Drug-eluting stents for the treatment of coronary artery disease; NICE Technology Appraisal Guidance, July 2008
- Percutaneous laser coronary angioplasty; NICE Interventional Procedure Guidance, January 2011
- Assessing fitness to drive: guide for medical professionals; Driver and Vehicle Licensing Agency
- Neumann FJ, Sousa-Uva M, Ahlsson A, et al; 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019 Jan 7;40(2):87-165. doi: 10.1093/eurheartj/ehy394.
About the authorView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
About the reviewerView full bio

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 7 Nov 2028
9 Nov 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in treatment and medication
- Acne treatments
- Anger management
- Anti-inflammatory tablets
- Anticoagulants
- Benzodiazepines and Z drugs
- Buprenorphine replacement for heroin
- Bupropion for quitting smoking
- Cancer treatment
- Drug allergy
- Epilepsy medication and side-effects
- Hot and cold therapy for pain relief
- Japanese encephalitis vaccine
- Medicines for urinary urgency and incontinence
- Nitrate medication
- Oral bronchodilators
- Sleeping tablets
- Steroid injections
- Steroid nasal sprays
- Steroids
- UpdatedTravel vaccinations