Cardiotocography
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Doug McKechnie, MRCGPLast updated 10 Oct 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Cardiotocography is usually called a 'CTG' by doctors and midwives. It can be used to monitor a baby's heart rate and a mother's contractions during labour.
Note: the information below is a general guide only. The arrangements, and the way tests are performed, may vary between different hospitals. Always follow the instructions given by your doctor or local hospital.
At a glance
Cardiotocography (CTG) measures your baby's heart rate and your womb's contractions.
It is used before and during labour to check for signs of a baby in distress.
External monitoring uses sensors on your tummy, while internal monitoring uses an electrode on the baby's scalp.
Healthcare professionals look at the baby's heart rate, its variability, and changes during contractions.
Regular CTG is usually advised if there are concerns about the pregnancy or the baby.
CTG is a safe test but can sometimes suggest a problem when there isn't one.
Internal monitoring may not be advised if you have certain infections.
Sign up for our free 8-week Healthy Pregnancy course!
Each week we’ll share useful information and essential tips on topics such as nutrition, exercise, mental health, symptoms to look out for, and preparing for childbirth, to help you navigate your pregnancy journey whatever stage you are at.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
In this article:
Continue reading below
What is cardiotocography?
Cardiotocography (CTG) measures your baby's heart rate. At the same time it also monitors the contractions in the womb (uterus). CTG is used both before birth (antenatally) and during labour, to monitor the baby for any signs of distress.
By looking at various different aspects of the baby's heart rate, doctors and midwives can see how the baby is coping.
The image below shows the equipment used to do a CTG. It normally stands by your bedside whilst you are being monitored.
CTG machine with printout
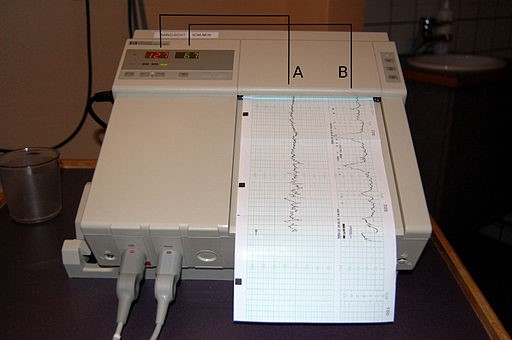
© Steven Fruitsmaak, CC BY 3.0, via Wikimedia Commons
What happens during cardiotocography?
Back to contentsExternal monitoring
CTG is most commonly carried out externally. This means that the equipment used to monitor the baby's heart is placed on the tummy (abdomen) of the mother.
An elastic belt is placed around the mother's abdomen. It has two round, flat plates about the size of a tennis ball which make contact with the skin. One of these plates measures the baby's heart rate. The other assesses the pressure on the tummy. In this way it is able to show when each contraction happens and an estimate of how strong it is. The midwife may put some jelly on the skin to help get a strong signal.
The CTG belt is connected to a machine which interprets the signal coming from the plates. The baby's heart rate can be heard as a beating or pulsing sound which the machine produces. Some mothers can find this distracting or worrying but it is possible to turn the volume down if the noise bothers you.
The machine also provides a printout which shows the baby's heart rate over a certain length of time. It also shows how the heart rate changes with your contractions.
If you have CTG before you are in labour you may be asked to press a button on the machine every time the baby moves. At this time you will not be having any contractions so the CTG will only monitor the baby's heart rate.
Internal monitoring
Occasionally during labour, if a signal can't be found using the external monitor, or when monitoring is more important, internal monitoring can be used.
For internal monitoring, a small, thin device called an electrode is used. This is inserted through the vagina and neck of the womb (which will be opening during labour) and placed on the baby's scalp. This device records the baby's heart rate.
If you have a twin (or higher multiples) pregnancy, internal monitoring can only be used on the baby closest to the neck of the womb.
Additionally internal monitoring can only be used when the baby is going to be delivered head first. Internal monitoring will not work on a breech (bottom or foot first) presentation.
Continue reading below
How does cardiotocography work?
Back to contentsCTG continually monitors the baby's heart rate and the mother's contractions.
External CTG monitoring uses ultrasound to detect the baby's heart rate. Ultrasound is a high-frequency sound that you cannot hear but it can be sent out (emitted) and detected by special machines.
In external CTG monitoring, a special type of ultrasound, called Doppler®, is used. This type of ultrasound is used to measure structures that are moving, making it useful for monitoring heart rate.
Internal CTG monitoring is slightly different. This uses a wire electrode, attached to the baby's scalp, to detect the electrical signals from the baby's heartbeat, measuring the heart rate that way.
The other plate on the CTG measures how tense the mother's tummy (abdomen) is. This measurement is used to show when the uterus is contracting.
What can cardiotocography show?
Back to contentsCTG is used to detect signs that the baby is in distress - for example, if it's not getting enough oxygen.
Many different things can be recorded on a CTG; your baby's heart rate, the baby's movements and your contractions. These are all shown on the image below.
CTG: electronic fetal monitoring machine
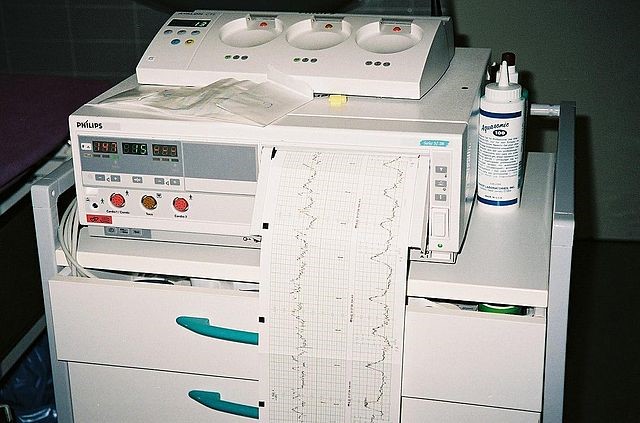
© LosHawlos, (GFDL) (CC-BY-SA), via Wikimedia Commons
Healthcare professionals look at different things on the CTG to get an overall picture of how the baby is doing. There are several different things for them to consider, including:
The baby's heart rate. A normal heart rate for a baby during labour is between 110 to 160 beats a minute. If the baby's heart rate is persistently low or high, this can suggest a problem.
The variability, or fluctuations, in the baby's heart rate. It's a good sign if the baby's heart rate changes slightly between beat-to-beat - this suggests that their brain is working well. If their heart rate stays very similar for a long time, this can suggest a problem.
Patterns of heart rate changes in the baby, in response to contractions.
The baby's heart rate increasing for a short time, and then going back to normal (called an acceleration) is a reassuring sign.
The baby's heart rate can also decrease for short periods (called a deceleration). This is normal if it happens during the beginning of contraction, and goes back to normal straight after the contraction. However, if they are happening without contractions, happening late in a contraction or are lasting a long time after the contraction finishes, they can be a sign that the baby is in difficulty.
Healthcare professionals will use all of this information to interpret the CTG results. They will decide if the CTG results are:
Reassuring - no signs of problems with the baby.
Suspicious - some signs that the baby is in distress.
Pathological - signs that strongly suggest the baby is in distress.
If the results are suspicious or pathological, clinicians will assess further and try to correct anything that could be affecting the baby. If this doesn't work, or if the CTG suggests that the baby is in serious distress, they are likely to recommend delivering the baby straight away for its safety. This might be using forceps or a ventouse (vacuum cup), or via a Caesarean section.
Continue reading below
What is cardiotocography used for?
Back to contentsIn a low-risk delivery, CTG is not usually needed. The midwife will listen to your baby's heart rate from time to time to check it is normal. However, in certain situations, continual monitoring with CTG is advised.
There are a lot of different possible reasons why CTG monitoring might be recommended. Generally, they are situations when close monitoring of the baby is thought to be needed to detect any problems.
The following are some examples:
Your baby is coming early or seems smaller than expected.
You have high blood pressure.
You have a high temperature (fever).
You have an infection.
You pass fresh blood whilst in labour.
You are expecting more than one baby (twins or more).
The baby has opened its bowels (passed meconium) into the amniotic fluid.
The midwife thinks there may be a problem, having listened with a Pinard® or Doppler® machine.
If your membranes have ruptured more than 24 hours before your labour starts.
If your baby is in an unusual position.
You have labour speeded up with Syntocinon® or need an epidural for pain relief.
If you have an epidural for pain relief during labour, CTG may be used for half an hour after an epidural has been put in, or after top-ups for the epidural.
There are other reasons as well.
Depending on the exact situation, some women may have continuous (ongoing) CTG monitoring. In other cases, women might have the CTG on for a short time only, and have it removed if the trace is normal.
Are there any side-effects or complications from cardiotocography?
Back to contentsCTG does not use any radiation; it is considered a very safe test. Depending on the machine used, it may prevent you from being able to move around freely during labour. Waterproof machines can be used in a water birth, but may not be available.
The aim of using CTG is to pick up signs that the baby is in trouble, allowing doctors and midwives to deliver the baby sooner, to prevent the baby from coming to harm.
However, like any test, CTG can sometimes be wrong. It can give 'false positives' - signs that the baby is in trouble, when it's actually not - leading to interventions (such as a forceps or Caesarean section) which are not really needed.
For this reason, CTG monitoring is usually not recommended for women who have no risk factors for birth complications, and no other signs that the baby is in trouble, as it's more likely to give false positives in this situation. Other forms of monitoring, like checking the baby's heartbeat every 15 minutes, is often recommended instead. It's a better test when used in women with higher-risk pregnancies.
Women who have infections such as herpes, hepatitis B or C or HIV do not usually have internal monitoring, as it may increase the chance of passing the infection on to the baby.
Patient picks for General pregnancy information

Pregnancy
Infertility treatments
Fertility treatment may be with medicines, with surgical operations, or by the use of assisted conception techniques, such as IVF.
by Dr Doug McKechnie, MRCGP

Pregnancy
Early pregnancy signs and symptoms
Pregnancy tests are very sensitive so it is common to find out that you are pregnant before you develop any signs or symptoms of pregnancy. However, as your pregnancy continues you may experience these early symptoms and signs of pregnancy. For further advice about having a healthy pregnancy, see also the leaflet Planning to Become Pregnant, which includes information about prenatal vitamin recommendations.
by Dr Colin Tidy, MRCGP
Sign up for our free 8-week Healthy Pregnancy course!
Each week we’ll share useful information and essential tips on topics such as nutrition, exercise, mental health, symptoms to look out for, and preparing for childbirth, to help you navigate your pregnancy journey whatever stage you are at.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Frequently asked questions
Can I request a CTG if I am not considered high-risk?
CTG monitoring is typically not recommended for women without risk factors for birth complications. In these cases, other forms of monitoring, such as checking the baby's heartbeat periodically, are usually suggested. This is because CTG may produce 'false positives' in low-risk situations, leading to unnecessary interventions.
What if I find the sound of my baby's heartbeat from the CTG machine distracting?
The CTG machine produces a beating or pulsing sound of your baby's heart rate. If you find this distracting or worrying, it is usually possible to turn the volume down to a more comfortable level.
Can I move around if I am having continuous CTG monitoring?
Depending on the specific CTG machine being used, continuous monitoring may limit your ability to move around freely during labour. Some waterproof machines exist and can be used during a water birth, but these might not always be available.
How do healthcare professionals interpret the CTG results?
Healthcare professionals consider various factors to get an overall picture of the baby's well-being. They look at the baby's heart rate, its variability (fluctuations), and how the heart rate changes in response to contractions. Based on these observations, the results are classified as 'reassuring', 'suspicious', or 'pathological'.
If my CTG results are 'suspicious' or 'pathological', what happens next?
If the CTG results are suspicious or pathological, clinicians will conduct further assessments to understand and address any potential issues. If these measures do not improve the situation, or if the CTG indicates severe distress, they may recommend delivering the baby promptly for its safety. This might involve methods such as forceps delivery, ventouse (vacuum cup), or a Caesarean section.
Further reading and references
- Intrapartum care; NICE Quality Standard, December 2015 - last updated February 2017
- Grivell RM, Alfirevic Z, Gyte GM, et al; Antenatal cardiotocography for fetal assessment. Cochrane Database Syst Rev. 2015 Sep 12;(9):CD007863. doi: 10.1002/14651858.CD007863.pub4.
- Alfirevic Z, Devane D, Gyte GM, et al; Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst Rev. 2017 Feb 3;2:CD006066. doi: 10.1002/14651858.CD006066.pub3.
- Fetal monitoring in labour; National Institute for Health and Care Excellence (NICE) [NG229]. December 2022.
Continue reading below
About the authorView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 9 Oct 2027
10 Oct 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in pregnancy
- Caesarean section
- Cot death
- Diaphragms and caps
- Epilepsy and planning pregnancy
- Feeding your baby
- Fetal anticonvulsant syndrome
- Infertility treatments
- Intrauterine contraceptive device
- Left lower quadrant pain in pregnancy
- Migraine and combined hormonal contraception
- Miscarriage and bleeding in early pregnancy
- Necrotising enterocolitis
- Ovulation calculator
- Pain relief in labour
- Pre-eclampsia
- Premature labour
- Progestogen-only contraceptive pill
- Retinopathy of prematurity
- Tear duct blockage in babies
- Urine infection in pregnancy