Femoral nerve lesion
Peer reviewed by Dr John Cox, MRCGPLast updated by Dr Roger Henderson, MBBSLast updated 20 Aug 2015
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
This page has been archived.
It has not been reviewed recently and is not up to date. External links and references may no longer work.
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article:
Damage to the femoral nerve may result from trauma, iatrogenically, or as a consequence of disease processes. Disruption may be complete or partial.
Continue reading below
Epidemiology
Femoral nerve lesions are uncommon. One study of 27,004 primary hip arthroplasties found only two patients with complete and one with partial femoral nerve palsy1. A review of cases treated surgically at a neurosurgical department found 119 patients over a period of 33 years. 52 cases were iatrogenic, 19 were due to hip or pelvic fractures, 10 to gunshot wounds and 8 to lacerations. The remainder were the result of various tumours or cysts2.
Causes3
Back to contentsIatrogenic:
Trauma - hip or pelvic fractures, thigh lacerations (these are often partial lesions, affecting nerve supply to the quadriceps).
Psoas haematoma - can occur as a complication of anticoagulant therapy or in haemophilia.
Psoas abscess6.
Diabetic amyotrophy (proximal neuropathy, seen in patients with diabetes, causes burning pain in the hip and thigh and wasting of thigh muscles)7.
Tumours - a variety of benign and malignant tumours - eg:
Arthropathy - femoral nerve palsy secondary to synovitis of the hip joint10.
Neonatal - femoral nerve palsy has been reported after breech lie in utero11.
Continue reading below
Presentation
Back to contentsSymptoms12
There may be instability of the knee (often described as 'buckling') on climbing stairs. The weakness is typically acute or subacute, in contrast to that caused by myopathy, in which the onset is often gradual and usually bilateral. Numbness of the medial side of the leg and calf may occur. Involvement of the lateral cutaneous branch of the nerve may produce painful paraesthesiae of the thigh (meralgia paraesthetica). Mild pain near the inguinal ligament may be experienced. Acute severe pain in the groin, thigh and lower abdomen may occur if the cause is a retroperitoneal haematoma.
Signs12
These may include:
Quadriceps muscle weakness and wasting.
Loss of knee jerk.
Numbness along the medial side of the thigh and anteromedial side of the calf (the L2-L4 dermatomes).
Pain on hip extension (in cases of retroperitoneal haematoma).
In one small study after gynaecological surgery, diagnosis was made based on the following criteria13:
History of falling during postoperative ambulation.
Quadriceps weakness.
Straight leg raise weakness.
Diminished knee jerk response.
No evidence of psoas haematoma or abscess.
Neurological Examination
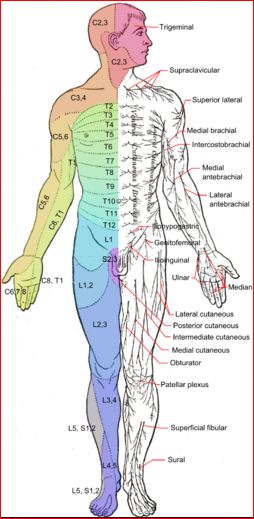
© Häggström, Mikael (2014). "Medical gallery of Mikael Häggström 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.008. ISSN 2002-4436. Public Domain
Differential diagnosis1415
Back to contentsFocal muscular atrophies
HIV-1-associated multiple mononeuropathies.
Inclusion body myositis (a group of hereditary disorders causing muscle weakness in which inclusion bodies are seen on microscopy of muscle cells).
Leptomeningeal carcinomatosis.
Metabolic myopathies.
Vasculitic neuropathy.
Lumbar plexopathies (peripheral neuropathy in the area of the lumbar plexus).
Lumbosacral disc syndromes.
Continue reading below
Investigations12
Back to contentsImaging
A CT scan of the abdomen may help to exclude retroperitoneal haematoma if this is suspected. CT or MRI imaging of the pelvis may also help to elucidate the cause (eg, tumour or aneurysm).
Other tests
Nerve conduction studies may reveal motor deficit.
Electromyography may show quadriceps weakness. Iliopsoas involvement may be demonstrated in pelvic lesions (ie the inguinal ligament).
Management16
Back to contentsMedical
Most patients can be treated conservatively with exercises, avoidance of excessive external rotation and abduction of the hip and with knee bracing.
Medical treatment depends on the underlying cause and this may include chemotherapy for an underlying tumour, immunotherapy for a diabetic or vasculitic cause and neuropathic pain medication (eg, pregabalin, gabapentin, amitriptyline).
The successful use of permanent percutaneous femoral nerve stimulation using a stimulating lead placed close to the femoral nerve with the aid of ultrasound guidance has been reported17.
Surgical
Surgical procedures which may be required include:
Drainage of a psoas haematoma or abscess18.
Treatment of a tumour.
Surgical decompression of the nerve.
Surgical exploration for other reasons (eg, penetrating wounds)2.
Nerve grafting after tumour excision19.
Successful transfer of the obturator nerve to the femoral nerve has been reported20.
Prognosis
Back to contentsPrognosis depends on the underlying cause. Most cases resolve spontaneously or with the aid of physical therapy. Symptoms caused by compression or stretching (eg, obstetric) can take three to four months to settle. Some patients are left with permanent residual neurological deficits21.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Kurt S, Kaplan Y, Karaer H, et al; Femoral nerve involvement in diabetics. Eur J Neurol. 2009 Mar;16(3):375-9.
- Retroperitoneal Hematoma with Femoral Nerve Damage; Nucleus Medical Media
- Farrell CM, Springer BD, Haidukewych GJ, et al; Motor nerve palsy following primary total hip arthroplasty. J Bone Joint Surg Am. 2005 Dec;87(12):2619-25.
- Kim DH, Murovic JA, Tiel RL, et al; Intrapelvic and thigh-level femoral nerve lesions: management and outcomes in 119 surgically treated cases. J Neurosurg. 2004 Jun;100(6):989-96.
- Head KA; Peripheral neuropathy: pathogenic mechanisms and alternative therapies. Altern Med Rev. 2006 Dec;11(4):294-329.
- Pechter EA, Smith PB; Transient femoral neuropathy after abdominoplasty. Ann Plast Surg. 2008 Nov;61(5):492-3.
- Barcin C, Kursaklioglu H, Kose S, et al; Transient femoral nerve palsy after diagnostic coronary angiography. Anadolu Kardiyol Derg. 2009 Jun;9(3):248-9.
- Atkinson C, Morris SK, Ng V, et al; A child with fever, hip pain and limp. CMAJ. 2006 Mar 28;174(7):924.
- Idiculla J, Shirazi N, Opacka-Juffry J, et al; Diabetic amyotrophy: a brief review. Natl Med J India. 2004 Jul-Aug;17(4):200-2.
- Stuplich M, Hottinger AF, Stoupis C, et al; Combined femoral and obturator neuropathy caused by synovial cyst of the hip. Muscle Nerve. 2005 Oct;32(4):552-4.
- Tajima Y, Sudoh K, Matsumoto A, et al; Femoral neuropathy induced by a low-grade myofibroblastic sarcoma of the groin. J Neurol. 2005 Nov;252(11):1416-7. Epub 2005 Jun 27.
- Tatsumura M, Mishima H, Shiina I, et al; Femoral nerve palsy caused by a huge iliopectineal synovitis extending to the iliac fossa in a rheumatoid arthritis case. Mod Rheumatol. 2008;18(1):81-5. Epub 2008 Jan 5.
- Szalay EA; Femoral nerve palsy and hip instability in infants with breech birth presentation: a review of the literature and report of 2 cases. J Pediatr Orthop. 2010 Oct-Nov;30(7):739-41.
- Felice KJ; Focal neuropathies of the femoral, obturator, lateral femoral cutaneous and other nerves of the thigh and pelvis. In: Bromberg MB, Smith GA,eds. Handbook of Peripheral Neuropathy. Boca Raton,FI: Taylor and Francis; 2005: chapter 31.
- Fanning J, Carol T, Miller D, et al; Postoperative femoral motor neuropathy: diagnosis and treatment without neurologic consultation or testing. J Reprod Med. 2007 Apr;52(4):285-8.
- Goyal N et al; Neuropathies - Weakness: Guidelines for a Cost-Effective Workup, ConsultantLive, 2007
- Goyal N et al; Myopathies - Weakness: Guidelines for a Cost-Effective Workup, ConsultantLive, 2007
- Ducic I, Dellon L, Larson EE; Treatment concepts for idiopathic and iatrogenic femoral nerve mononeuropathy. Ann Plast Surg. 2005 Oct;55(4):397-401.
- Narouze SN, Zakari A, Vydyanathan A; Ultrasound-guided placement of a permanent percutaneous femoral nerve stimulator leads for the treatment of intractable femoral neuropathy. Pain Physician. 2009 Jul-Aug;12(4):E305-8.
- Parmer SS, Carpenter JP, Fairman RM, et al; Femoral neuropathy following retroperitoneal hemorrhage: case series and review of the literature. Ann Vasc Surg. 2006 Jul;20(4):536-40. Epub 2006 May 31.
- Tsuchihara T, Nemoto K, Arino H, et al; Sural nerve grafting for long defects of the femoral nerve after resection of a retroperitoneal tumour. J Bone Joint Surg Br. 2008 Aug;90(8):1097-100.
- Campbell AA, Eckhauser FE, Belzberg A, et al; Obturator nerve transfer as an option for femoral nerve repair: case report. Neurosurgery. 2010 Jun;66(6 Suppl Operative):375; discussion 375.
- Moore AE, Stringer MD; Iatrogenic femoral nerve injury: a systematic review. Surg Radiol Anat. 2011 Feb 17.
Continue reading below
About the authorView full bio

Dr Roger Henderson, MBBS
General Practitioner, Medical Author
MBBS, LMSSA
Dr Roger Henderson qualified as a GP in 1985 and has authored for EMIS since early 2013.
About the reviewerView full bio

Dr John Cox, MRCGP
MA, MB, B Chir, DCH, DRCOG, MRCP (UK), MRCGP
Dr John Cox worked as a Medical Registrar in the UK and New Zealand and as a locum Physician in New Zealand.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
20 Aug 2015 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
More in history and examination
- Abdominal examination
- Abdominal pain in pregnancy
- Abnormal weight loss
- UpdatedAscites
- Dehydration in children
- Fatigue and TATT
- Fungal nail infections
- Generalised lymphadenopathy
- Healthy child programme
- Horner's syndrome
- Mononeuropathies
- Mother's six-week postnatal check
- Night terrors and parasomnias
- Orbital swellings
- Paediatric history
- Palmar erythema
- Pigmented purpuric dermatosis
- Post-inflammatory hyperpigmentation of skin
- Right iliac fossa pain
- Voiding difficulties