Appendicitis
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Colin Tidy, MRCGPLast updated 10 Feb 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Symptoms of appendicitis
Appendicitis is inflammation of the appendix, a small pouch on the gut wall connected to the large intestine. It is a medical emergency as, left untreated, the appendix can burst or perforate.
At a glance
The appendix is a small, blind-ended tube off the large bowel, usually in the lower right tummy.
Common symptoms include pain that moves to the lower right tummy, feeling sick, and a high temperature.
Appendicitis is common and can affect anyone, though it is most common between ages 10 and 30.
If appendicitis is suspected, early treatment is needed to prevent it from bursting, which is very serious.
Treatment usually involves an operation to remove the appendix, often through keyhole surgery.
In this article:
Video picks for Abdominal pain
Continue reading below
What is the appendix?
The appendix is a small, blind-ended tube that comes off the caecum, which is the very first part of the large bowel (large intestine). In the vast majority of people the appendix is located in the bottom, right-hand quarter of the tummy.
The appendix is normally about 5-10 cm long, but quite narrow. It has muscular walls, like the intestine, and there is some immune tissue in those walls. Scientists used to believe that the appendix had no useful role in modern humans. They thought that our ancestors had needed the appendix only to digest tough food like tree bark. However, more recently it has been suggested that the appendix may contain a reservoir of helpful digestive bacteria and that, in early childhood, the immune tissues in the appendix are important in the development of the immune system. Despite all this it seems that removing the appendix leaves no ill effects.
What causes appendicitis?
Back to contentsAppendicitis is thought most often to be caused by blockage of the appendix 'tube' either by something stuck on the inside, or by swelling of the appendix wall. Blockage may be by trapped seeds, indigestible food remnants or hard stools (faeces) that get stuck in the appendix, or by lymph glands in the appendix wall which have swollen in response to signs of infection elsewhere in the body.
If the appendix is inflamed and swollen, and cannot empty, then germs (bacteria) may thrive and cause inflammation in the wall and behind the blockage in the 'dead end' of the appendix.
Can stress cause appendicitis?
There is no evidence to suggest that stress can cause appendicitis. However it has been suggested that long-term stress can affect the normal function of the bowel and also reduce defences to infection (immunity), and so be a factor in causing appendicitis.
Continue reading below
How common is appendicitis?
Back to contentsAppendicitis is common and can affect anyone of any age. Teenagers and young adults are the most commonly affected.
About 1 in every 7 people in the UK have appendicitis at some time in their lives. Appendicitis can develop at any age but it is most common between ages 10 and 30. It is very rare under the age of 2 years.
It is slightly more common in women than in men and is much more common in western countries. This is thought to be partly due to the western diet which is often low in fibre. It is rare in rural parts of the developing world.
Appendicitis symptoms
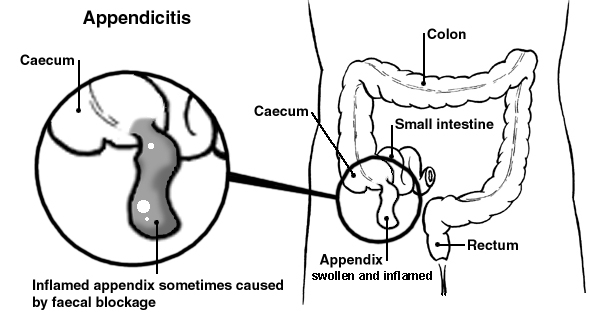
Back to contentsDiagram of the bowel showing an inflamed appendix
The common symptoms of appendicitis include:
Pain, often starting as a dull ache around the tummy button, getting worse and more constant over several hours and moving to the lower right tummy.
Loss of appetite.
High temperature (fever).
Bloating.
Appendicitis is painful, although the severity of the pain can vary. The inflamed appendix becomes infected with germs (bacteria) from the intestine. Once it becomes inflamed, the appendix gradually swells and fills with pus.
Eventually, if not treated, the swollen appendix becomes weakened, and can burst (perforate). A burst appendix is very serious, as the contents of the intestine can then leak into the abdominal cavity (tummy). Here they may cause a serious infection of the membrane that lines the abdomen (a condition called peritonitis), or a collection of pus (an abscess) in the abdomen. So, if appendicitis is suspected, early treatment is needed before it bursts.
The signs of appendicitis in children often differ from those seen in adults, to learn more about the specific symptoms in children, read our article Appendicitis in children: what are the signs?
Continue reading below
How is appendicitis diagnosed?
Back to contentsA doctor may diagnose appendicitis quite easily if you have the typical appendicitis symptoms. However, not everyone has typical symptoms of appendicitis.
There is no easy, foolproof test that can confirm appendicitis. A surgeon often has to make the final judgement about whether to operate, based on their assessment of you. It therefore depends on whether your symptoms, and the findings when you are examined, suggest that appendicitis is the probable diagnosis.
Abdominal examination
Your tummy (abdomen) will be examined to assess where you are tender. This includes pushing into the tender areas to see if your muscles can relax, and where you are most tender. Blood tests may also help when diagnosing appendicitis.
Urine testing
Urine testing is done to rule out a urinary tract infection, and women are usually offered pregnancy tests.
Imaging tests
Imaging tests are often used to help decide on the diagnosis, if it is not clear. For example, an ultrasound scan or a computerised tomography (CT) scan may help to clarify the cause of the symptoms. If the diagnosis seems obvious or there is concern that your appendix has, or is about to, burst (perforate), you are likely to go straight to surgery. This will avoid the delay caused by taking you for a scan first.
Monitoring
Sometimes a surgeon advises to wait and see for a few hours or so while you are being monitored in hospital. This allows some time to see if your symptoms progress to a more definite diagnosis, or even if they change or go away. Antibiotic medicine will usually be given in this time.
What else could it be?
Back to contentsSome people develop abdominal pain that is similar to appendicitis symptoms but which is caused by other conditions. For example:
Urinary tract infection (cystitis).
Passing a kidney stone (ureteric colic).
Inflammation of the large bowel (large intestine) - a condition called colitis.
Inflammation of the first part of the large bowel (the caecum) itself - sometimes seen in Crohn's disease.
In women the right ovary lies near to the appendix, so pain in this area could come from either organ. A leaking ovarian cyst, or the normal pain of ovulation (sometimes called Mittelschmerz) can mimic appendicitis.
Ectopic pregnancy (when a pregnancy starts to develop outside the womb, usually in one of the Fallopian tubes) can mimic appendicitis.
In children swollen glands in the tummy around the bowel (mesenteric adenitis), often associated with viral infections can mimic appendicitis.
Occasionally pain from gallstones or from inflammation of the gallbladder (cholecystitis) can mimic appendicitis.
Some people have surgery only to find that the appendix is normal and not inflamed.
Appendicitis treatment
Back to contentsThe normal, established way to treat appendicitis is an operation to remove the inflamed appendix. The aim is to do this before it bursts (perforates), as a perforated appendix is a very serious condition.
Surgery to remove the appendix
In a surgical removal of the appendix, the inflamed appendix is found and cut off at the first part of the large bowel (large intestine) - the caecum. The hole this leaves in the caecum is stitched up to stop contents from the gut leaking out. Antibiotic medicine is given before surgery to reduce the risk of infection developing at the site of the operation.
Sometimes antibiotics are used to delay surgery until the appendicitis has calmed a little. This may make the surgery safer and reduces the risk that the appendix will burst at operation.
Removal of the appendix is one of the most commonly performed operations in the UK. This is usually a straightforward and successful operation with a short recovery time. Surgery is commonly done by a keyhole operation, as the recovery is quicker compared to having an open operation. The keyhole operation is performed through three tiny cuts, the largest of which is only around 1.5 cm in size.
Sometimes keyhole surgery isn't recommended and open surgery on the tummy (abdomen) area is performed instead. This is likely to be needed if the appendix has already burst and caused a severe abdominal infection (peritonitis) or formed a lump called an appendix mass. It is also more likely if:
You have had other abdominal surgery and have scarring.
During the keyhole surgery a blood vessel is damaged by the instruments and needs repair.
Your appendix is not situated in the usual place.
You are pregnant.
There are usually no long-term complications with appendicitis after the operation. As with any operation, there is a small risk of complications from the operation itself (including bleeding and infection) and from the anaesthetic. You will usually be able to go home within 24 hours of uncomplicated surgery. You can expect some pain, and often constipation, but these should start to improve within a few days. You should be able to resume your normal activities a couple of weeks after keyhole surgery.
However, if you don't have an operation, an inflamed appendix is likely to burst and cause peritonitis. This can be life-threatening. Untreated burst appendix with peritonitis has caused many deaths in history. The famous magician, Harry Houdini, used to invite members of the audience to punch him in the stomach to demonstrate his strong abdominal muscles. Unfortunately, someone did this when he was unprepared. Even more unhappily, he had appendicitis at the time. His appendix burst and this resulted in his death some hours later.
Treatment of an appendix mass
If an appendix mass has formed then surgeons sometimes suggest postponing surgery whilst they drain the mass and treat with antibiotics, before doing a full appendicectomy a few weeks later. This allows patients to have surgery when they are less unwell, and the surgery is less difficult, as the inflammation has started to settle.
Antibiotics for appendicitis
Back to contentsSome studies have suggested that in some cases of appendicitis, it can be treated with antibiotics alone, without the need for surgery. This removes the risks associated with surgery. However, larger studies have not supported the use of antibiotics instead of surgery and so antibiotic treatment is not recommended for routine practice.
Dr Mary Lowth is an author or the original author of this leaflet.
Patient picks for Abdominal pain

Digestive health
Mesenteric adenitis
Mesenteric adenitis means swollen (inflamed) lymph glands in the tummy (abdomen), which causes tummy pain. It is sometimes called mesenteric lymphadenitis. The mesentery is the part of the tummy where the glands are located. Adenitis means inflamed lymph glands.
by Dr Doug McKechnie, MRCGP

Digestive health
Left upper quadrant pain
Left upper quadrant (LUQ) pain is pain located in the upper part of the abdomen on your left-hand side. There are many causes of LUQ pain.
by Dr Hayley Willacy, FRCGP
Frequently asked questions
What is the appendix's purpose in the body?
The appendix is a small, tube-like organ attached to the large bowel. While it was once thought to have no useful role, recent suggestions indicate it may store helpful digestive bacteria and that its immune tissues are important for immune system development in early childhood. Despite these potential roles, its removal doesn't cause any known ill effects.
How does appendicitis start?
Appendicitis most commonly begins when the appendix becomes blocked. This blockage can be caused by various things, such as trapped seeds, undigested food particles, or hardened stools. Swelling of lymph glands in the appendix wall, often in response to an infection elsewhere in the body, can also lead to a blockage. Once blocked, bacteria can thrive inside, leading to inflammation and swelling.
Can I prevent appendicitis?
The article suggests that appendicitis is more common in Western countries, partly due to a diet often low in fibre. While it doesn't offer explicit prevention methods, maintaining a high-fibre diet might be a factor to consider given this information.
Are new treatments available for appendicitis besides surgery?
The standard treatment for appendicitis is surgical removal. While some studies have explored treating certain cases with antibiotics alone to avoid surgical risks, larger studies have not supported this approach for routine practice. Therefore, surgery remains the recommended primary treatment.
What happens if appendicitis is not treated?
If left untreated, an inflamed appendix will likely rupture (burst or perforate). This is a very serious condition because the contents of the intestine can then leak into the abdominal cavity, leading to a severe infection of the abdominal lining called peritonitis, or the formation of a pus collection (an abscess). These complications can be life-threatening.
Further reading and references
- Jaschinski T, Mosch CG, Eikermann M, et al; Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev. 2018 Nov 28;11:CD001546. doi: 10.1002/14651858.CD001546.pub4.
- Becker P, Fichtner-Feigl S, Schilling D; Clinical Management of Appendicitis. Visc Med. 2018 Dec;34(6):453-458. doi: 10.1159/000494883. Epub 2018 Nov 24.
- Appendicitis; NICE CKS, May 2021 (UK access only)
- Baird DLH, Simillis C, Kontovounisios C, et al; Acute appendicitis. BMJ. 2017 Apr 19;357:j1703. doi: 10.1136/bmj.j1703.
- Herrod PJJ, Kwok AT, Lobo DN; Randomized clinical trials comparing antibiotic therapy with appendicectomy for uncomplicated acute appendicitis: meta-analysis. BJS Open. 2022 Jul 7;6(4):zrac100. doi: 10.1093/bjsopen/zrac100.
Continue reading below
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 9 Feb 2028
10 Feb 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.