Throat cancer
Laryngeal cancer
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 15 Jun 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Most cases of cancer of the voice box (larynx) occur in people aged over 60. The common early symptom is a persistent hoarse voice. Many cases are diagnosed at an early stage when there is a good chance of a cure. In general, the more advanced the cancer (the more it has grown and spread), the less chance that treatment will be curative.
At a glance
Throat cancer is a general term for cancers affecting the throat, including laryngeal cancer.
Squamous cell carcinoma of the larynx is the most common type, affecting over 9 in 10 cases.
A persistent hoarse voice for 2-4 weeks should be checked by a doctor.
Smoking and drinking large amounts of alcohol increase the risk.
Treatment options include radiotherapy, surgery, and chemotherapy.
Early diagnosis and treatment offer a good chance of a cure.
What is throat cancer?
Throat cancer is a general term used to describe cancers of the throat. It is sometimes called laryngeal cancer (cancer of the larynx). However, the throat includes other nearby structures as well as the voice box (larynx).
Laryngeal cancer is just one type of cancer that can occur in the throat. Throat cancers and cancers that affect the mouth, are together all called oropharyngeal cancers.
How common is throat cancer?
Throat (laryngeal) cancer is uncommon in the UK with around 2,000 cases developing each year. It is twice as common in men as in women. Although it is increasing in younger people it is still rare in people aged under 40 years. It is most common in people aged over 70 years. Cancer of the larynx occurs in people all over the world but is more common is some countries than in others, probably due to exposure to known risk factors (see below).
Types of throat cancer
There are different types of throat (laryngeal) cancer:
Squamous cell carcinoma of the larynx occurs in more than 9 in 10 cases. This type arises from cells which are on the inside lining of the larynx.
Other types. There are some rare types of cancer which arise from other types of cells within the larynx. For example, adenocarcinoma of the larynx arises from cells in the tiny glands in the wall of the larynx that make mucus. There are some other very rare types.
See the separate leaflet called Cancer for more general information about cancer
The rest of this leaflet is about squamous cell carcinoma of the larynx.
What is the larynx?
Head and neck showing larynx
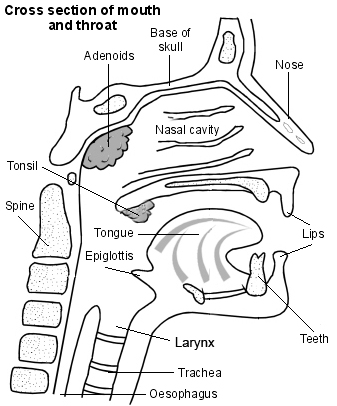
The larynx makes up part of the throat and is located at the top part of the windpipe (trachea). It is about 5 cm long and is sometimes called the voice box. You can see and feel the front part of the larynx as the Adam's apple on the front of the neck, just below the chin.
The larynx contains the vocal cords. These are V-shaped ridges of muscle tissue on the inside lining of the larynx. They vibrate when air passes between them to produce speech. This is why the larynx is also called the voice box.
When you breathe in, air passes into the larynx and down the trachea towards the lungs. When you swallow, the larynx moves upwards slightly and a flap of cartilage tissue at the back of the tongue, called the epiglottis, closes over the entrance to the larynx. This ensures that food or drink goes down the gullet (oesophagus) and not down the trachea.
Throat cancer symptoms
A hoarse voice is often the first symptom because most cancers of the larynx first start on, or close by, a vocal cord. The problem is a hoarse voice is a common symptom of a viral infection of the larynx (laryngitis). Most people with hoarseness do not have cancer. However, laryngitis usually clears within a week or so. Therefore, see a doctor if you develop a hoarse voice which does not go within 2-4 weeks.
Other symptoms that may occur as the tumour grows in the larynx include: a lump in the throat, a sore throat when swallowing, and difficulty with breathing. These symptoms may occur before a hoarse voice develops if the tumour does not start next to the vocal cords.
If the cancer spreads to local lymph glands (lymph nodes) then the nearby glands in the neck will swell.
If the cancer spreads to other parts of the body, various symptoms can develop.
Unexplained weight loss.
All the symptoms can be due to other conditions, so tests are needed to confirm the diagnosis
Causes of throat cancer
A cancerous (malignant) tumour starts from one cell behaving abnormally. The exact reason why a cell does this is unclear. It is thought that something damages or changes certain genes in the cell. This makes the cell multiply out of control and become cancerous. See the separate leaflet called Causes of Cancer for more details.
Some people develop throat (laryngeal) cancer for no apparent reason. However, certain risk factors increase the chance that cancer of the larynx may develop. These include:
Smoking. The damaging smoke passes through the larynx on its way to the lungs. The more you smoke, the greater the risk:
Smoking at all makes you 10 to 15 times more likely to develop throat (laryngeal) cancer than a non-smoker.
If you smoke heavily (20 cigarettes or more a day) you are 30 times more likely to develop throat (laryngeal) cancer.
Regularly drinking large amounts of alcohol. The more you drink, the more likely you are to develop throat (laryngeal) cancer:
Drinking alcohol makes you about two and a half times more likely to develop throat (laryngeal) cancer, if you don't also smoke. It is much more likely if you smoke too.
Ageing. It is more common in older people. Most cases are in people over 70.
Human papillomavirus (HPV) is associated with cancer of the larynx:
People who develop HPV-associated cancer of the larynx tend to be younger and also tend to have a better outlook (prognosis).
Most people with HPV will not develop throat (laryngeal) or any other cancer.
There is an immunisation against HPV which may reduce the risk of developing cancer of the larynx. You can find out more about this in the separate leaflet called Human Papillomavirus Immunisation (HPV).
A poor diet may be a risk factor, especially a diet lacking in certain vitamins and minerals.
Long-term exposure to certain chemicals, fumes or pollutants may irritate the larynx if you breathe them in and may increase the risk.
Throat cancer diagnosis
Initial assessment
If a doctor suspects that you may have throat (laryngeal) cancer, they will refer you to an ear, nose and throat (ENT) specialist. The specialist will examine the inside of your throat by using a small mirror and light. They may also use a thin, flexible, telescope (a nasal endoscope).
This is passed into your nose and down the back of your throat. The nasal endoscope contains fibre-optic channels, allowing light to shine down so the doctor can see inside. (The throat is usually sprayed with a local anaesthetic before use of a nasal endoscope, so that the procedure is not too uncomfortable.)
Editor’s note
Dr Krishna Vakharia, 16th October 2023
The National Institute for Health and Care Excellence (NICE) has recommended that a person should receive a diagnosis or ruling out of cancer within 28 days of being referred urgently by their GP for suspected cancer.
To confirm the diagnosis
If anything suspicious is seen by the examination or with the nasal endoscope, you will usually need a biopsy. A biopsy is a procedure involving a small sample of tissue being removed from a part of the body. The sample is then looked at under the microscope to look for abnormal cells.
The biopsy sample is obtained by a thin, flexible grabbing instrument which is passed through your nose into the larynx. The same instrument has a light source similar to a nasal endoscope. Therefore, the specialist will also examine the windpipe (trachea) and the gullet (oesophagus) to see the extent of any tumour.
Assessing the extent and spread (staging)
In addition to the above tests, if you are confirmed to have throat (laryngeal) cancer then further tests may be done; for example, biopsy samples may be taken from the nearby lymph glands by using a fine needle. This helps to assess if any cancer cells have spread to the lymph glands.
Other tests may be arranged to see if the cancer has spread to other parts of the body. For example, a computerised tomography (CT) scan, a magnetic resonance imaging (MRI) scan, a positron emission tomography (PET) scan or other tests. (You can read more about these tests in the separate leaflets called CT scan, MRI scan and PET scan.)
This assessment is called staging of the cancer. The aim of staging is to find out:
How much the tumour in the larynx has grown.
Whether the cancer has spread to local lymph nodes.
Whether the cancer has spread to other areas of the body (metastasised).
Grade of the cancer
The biopsy samples are looked at under the microscope to assess the cancer cells. By looking at certain features of the cells the cancer can be graded.
The common grading system used for throat (laryngeal) cancer is:
Grade 1 (low grade). The cells look reasonably similar to normal cells in the larynx. The cancer cells are said to be well differentiated. The cancer cells tend to grow and multiply quite slowly and are not so aggressive.
Grade 2 (intermediate grade).
Grade 3 (high grade). The cells look very abnormal and are said to be poorly differentiated. The cancer cells tend to grow and multiply quite quickly and are more aggressive.
By finding out the stage and grade of the cancer it helps doctors to advise on the best treatment options. It also gives a reasonable indication of outlook (prognosis). However, for throat (laryngeal) cancer, it may not be possible to give an accurate staging until after an operation to remove the tumour. See the separate leaflet called Stages of Cancer for more details.
Throat cancer treatment
Treatment options which may be considered include radiotherapy, surgery and chemotherapy. The treatment advised for you depends on various factors such as the exact site of the primary tumour in the larynx, the stage of the cancer (how large the cancer is and whether it has spread), the grade of the cancerous cells and your general health.
You should have a full discussion with a specialist who knows your case. They will be able to give the pros and cons, likely success rate, possible side-effects and other details about the possible treatment options for your type of cancer.
You should also discuss with your specialist the aims of treatment. For example:
In some cases, treatment aims to cure the cancer. There is a good chance of a cure if it is treated in the early stages. Many cases are diagnosed at an early stage. This is because tests are usually done if you develop a persistent hoarse voice which often develops when the cancer is still at an early stage. (Doctors tend to use the word remission rather than the word cured. Remission means there is no evidence of cancer following treatment. If you are in remission, you may be cured. However, in some cases a cancer returns months or years later. This is why doctors are sometimes reluctant to use the word cured.)
In some cases, treatment aims to control the cancer. If a cure is not realistic, with treatment it is often possible to limit the growth or spread of the cancer so that it progresses less rapidly. This may keep you free of symptoms for some time.
In some cases, treatment aims to ease symptoms. For example, if a cancer is advanced then you may require painkillers or other treatments to help keep you free of pain or other symptoms. Some treatments may be used to reduce the size of a cancer, which may ease symptoms such as pain or difficulty with swallowing.
Radiotherapy
This is the common treatment if the cancer is small and has not spread from the larynx (early stage). Radiotherapy is a treatment which uses high-energy beams of radiation which are focused on cancerous tissue. This kills cancer cells, or stops cancer cells from multiplying. See the separate leaflet called Radiotherapy for more details.
Radiotherapy alone gives a good chance of a cure if the cancer is at an early stage. Radiotherapy is also sometimes used in addition to surgery or chemotherapy in certain situations. For example, radiotherapy may be used to shrink a large tumour prior to surgery. This may give a better chance of success with surgery. It is sometimes used following surgery, to kill any cancer cells which may have been left behind following the operation.
Surgery
Tumours which are larger tend to require surgery. Sometimes surgery is aimed at curing the cancer by removing it all. Sometimes surgery is used to relieve symptoms if the cancer is at an advanced stage (palliative surgery). The operations are all done whilst you are asleep under a general anaesthetic.
The type of operation done depends on the size of the tumour, the exact site of the tumour in the larynx and whether the cancer has spread to nearby structures or lymph glands. For example:
Endoscopic resection. This is a technique which can remove a small tumour in the larynx. Instruments which cut out a tumour are passed down the inside of the larynx. Sometimes a laser is used to burn out the tumour. This technique does not involve a cut from the outside. It is sometimes called transoral laser microscopic (TLM) surgery. It is only suitable for tumours that are small and still confined to the inner lining of the larynx.
Partial laryngectomy. This is an operation where the affected part of the larynx is cut out. A cut is made in the front of the neck to get at the larynx. If only part of the larynx is removed you should not need a permanent hole in the neck (stoma) to breathe and speech may be preserved. A temporary stoma may be required whilst the wound is healing.
A total laryngectomy. This is an operation where the entire larynx is removed. To be able to breathe after the operation, the top part of the windpipe (trachea) is attached to the front of the neck. You will then have a permanent stoma in the front of the neck. The vocal cords will have been removed so you will not be able to speak normally again. However, there are various techniques that you can be taught by a speech therapist which can enable you to make sounds and speak in a different way.
If the cancer has spread, the surgeon may also remove lymph glands and other structures near to the larynx in addition to removing the larynx. The amount of tissue removed depends on the extent of local spread of the cancer.
Chemotherapy
Chemotherapy is a treatment which uses anti-cancer drugs to kill cancer cells, or to stop them from multiplying. Chemotherapy used in conjunction with radiotherapy is sometimes used as an alternative to surgery. It aims to preserve the larynx and normal speech. Your specialist will advise when this may be an option. Chemotherapy may also be advised if the cancer has spread to other areas of the body.
Other treatments
Cetuximab is a fairly new treatment for throat (laryngeal) cancer. It is a type of monoclonal antibody which means that it can recognise and bind to specific proteins (receptors) that are found in the cancer cells. These proteins are epidermal growth factor receptors (EGFRs) which stimulate the cancer cell to grow and divide. Cetuximab locks on to the EGFR and can prevent the cancer cells from growing and dividing.
At the moment, cetuximab is a treatment that is usually given at the same time as radiotherapy in people who are unable to have chemotherapy.
Preventing throat cancer
Some of the risk factors that make laryngeal cancer more likely can be avoided. Reducing the number of risk factors you have will reduce the risk. Strategies include:
Reduce the amount of alcohol you drink.
Have a balanced diet.
Avoid exposure to chemicals, fumes or pollutants where possible.
What is the outlook of throat cancer?
If a throat (laryngeal) cancer is diagnosed and treated at an early stage then there is a good chance of a cure. A cure is less likely if the cancer has spread. Voice problems are extremely common after treatment for laryngeal cancer and speech therapy should be offered to anyone affected.
The treatment of cancer is an area of medicine that is developing quickly. New treatments are constantly being developed and the information on outlook (prognosis) above is very general. The specialist who knows you and your disease can give you more accurate information about your particular outlook and how your stage and grade of cancer is likely to behave with treatment.
Patient picks for Other cancer types

Cancer
Brain tumours
This leaflet aims to give a brief overview of the various types of brain tumours. The treatment and survival rates vary greatly, depending on factors such as the type of tumour and the location in the brain.
by Dr Toni Hazell, FRCGP

Cancer
Lung cancer
Lung cancer (cancer of the lung) is common worldwide. Around 4 in 10 cases develop in people over the age of 75 years, usually in smokers. If lung cancer is diagnosed at an early stage, there is a chance of a cure. In general, the more advanced the cancer (the more it has grown and spread), the less chance that treatment will be curative. However, treatment can often slow the progress of the cancer.
by Dr Colin Tidy, MRCGP
Frequently asked questions
What is the difference between diagnosing and staging throat cancer?
Diagnosis of throat cancer involves an initial examination by an ENT specialist, often using a small mirror and light or a nasal endoscope. If anything suspicious is found, a biopsy is performed to confirm the presence of cancer cells. Staging, on the other hand, determines the extent and spread of the confirmed cancer. This can involve additional tests like CT, MRI, or PET scans, and sometimes biopsies of nearby lymph glands, to assess tumour size, spread to lymph nodes, or to other parts of the body.
If I am diagnosed with throat cancer, how quickly can treatment begin?
The National Institute for Health and Care Excellence (NICE) recommends that a person should receive a diagnosis or ruling out of cancer within 28 days of being urgently referred by their GP for suspected cancer. Once diagnosed, a full discussion with a specialist will take place to determine the best treatment options based on your specific case.
What happens after a total laryngectomy if the vocal cords are removed?
If a total laryngectomy is performed, the entire larynx, including the vocal cords, is removed. This means you will not be able to speak normally again. However, you can be taught various techniques by a speech therapist to enable you to make sounds and speak in a different way.
What is the role of Cetuximab in treating throat cancer?
Cetuximab is a relatively new treatment for throat (laryngeal) cancer. It is a type of monoclonal antibody that specifically targets and binds to epidermal growth factor receptors (EGFRs) on cancer cells, which are proteins that stimulate cell growth. By locking onto these receptors, Cetuximab can prevent the cancer cells from growing and dividing. It is typically used in conjunction with radiotherapy for people who are unable to have chemotherapy.
Can I prevent throat cancer by getting vaccinated against HPV?
Yes, there is an immunisation against Human Papillomavirus (HPV) which may reduce the risk of developing laryngeal cancer. HPV is associated with some cases of laryngeal cancer, and these cases often have a better outlook. While most people with HPV do not develop cancer, vaccination can be one strategy to help reduce your risk.
Further reading and references
- Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over; NICE Guidance (February 2016 - last updated November 2018)
- Oral cancer incidence statistics; Cancer Research UK
- Syrjanen S, Rautava J, Syrjanen K; HPV in Head and Neck Cancer-30 Years of History. Recent Results Cancer Res. 2017;206:3-25. doi: 10.1007/978-3-319-43580-0_1.
- Koroulakis A, Agarwal M; Laryngeal Cancer.
- Cetuximab for treating recurrent or metastatic squamous cell cancer of the head and neck; NICE Technology appraisal guidance [TA473]. Published August 2017.
- Blomkvist R, Marklund L, Hammarstedt-Nordenvall L, et al; Treatment and outcome among patients with laryngeal squamous cell carcinoma in Stockholm-A population-based study. Laryngoscope Investig Otolaryngol. 2023 Mar 6;8(2):441-449. doi: 10.1002/lio2.1034. eCollection 2023 Apr.
- Andaloro C, Widrich J; Total Laryngectomy.
About the authorView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 12 May 2028
15 Jun 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in cancer
- Bone marrow biopsy and aspiration
- Breast cancer in men
- Breast screening
- Cancer symptoms
- Cancer treatment
- Cervical cancer
- Childhood leukaemias
- Diagnosing cancer
- Faecal immunochemical test
- Hodgkin's lymphoma
- Lung cancer
- Neuroblastoma
- Paget's disease of bone
- Pancreatic cancer
- Primary bone cancer
- Stages of cancer
- Stem cell transplant
- Stomach cancer
- Thyroid cancer
- Wilms' tumour