Breast cancer
Peer reviewed by Dr Rosalyn Adleman, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 31 Oct 2022
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
If you notice any lump or change to how your breast normally feels you should see a doctor promptly.
Breast cancer is the most common cancer in women. Most cases occur in women over the age of 50 but breast cancer can occur in younger women. If breast cancer is diagnosed at an early stage, less treatment may be needed and it is more likely to be effective . In general, the more advanced the cancer (the more it has grown and spread), the less chance that treatment will be curative.
However, treatments are improving all the time and they can often slow the progress of the cancer. Over 3 out of 4 women diagnosed with breast cancer are still alive 10 years later.
At a glance
Breast cancer is a common cancer, mainly affecting women over 50, but can occur in younger people and men.
Knowing your breasts and checking for changes is important.
Symptoms include a painless lump, changes in breast size or shape, dimpling skin, or a turned-in nipple.
If you notice a lump, always see a doctor promptly even if most lumps are not cancerous.
Various treatments are available, including surgery, chemotherapy, radiotherapy, and hormone therapy.
Early diagnosis of breast cancer significantly improves the chance of a cure.
What is breast cancer?
What is breast cancer?
Breast cancer is one of the most common cancers. Around one in nine women develop breast cancer at some stage in their lives. About 48,000 cases occur in the UK each year. Most develop in women over the age of 50 but younger women are sometimes affected. Breast cancer develops from a cancerous (malignant) cell which develops in the lining of a duct or lobule in one of the breasts.
Breast cancer can also develop in men, although this is much less common than breast cancer in women.
Anatomy of the breasts
Cross-section view of breast
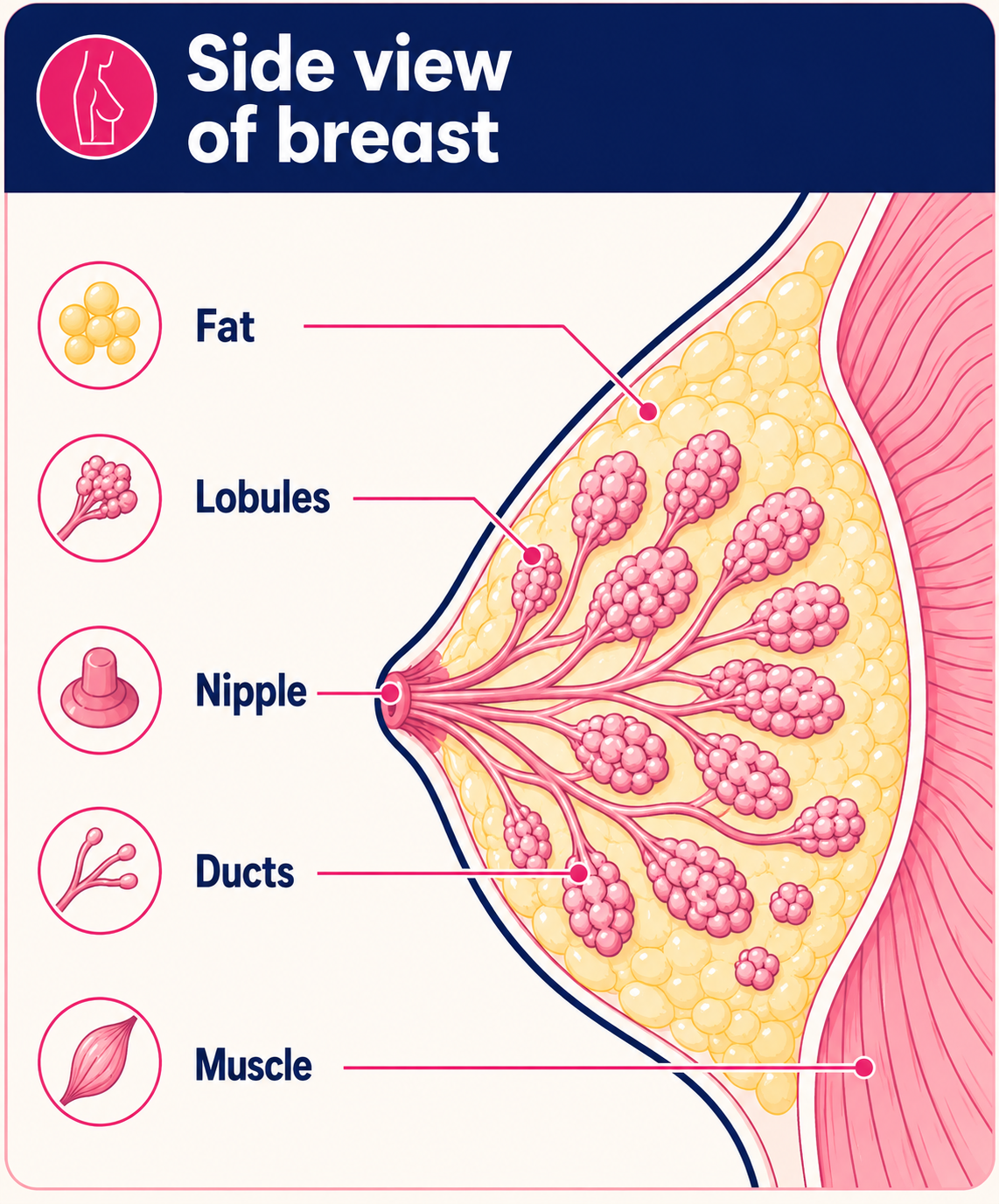
Breast tissue is attached to muscle on the chest wall. A tail of breast tissue extends up into the armpit. The breasts contain:
Many lobules which are made up of glandular tissue. They make milk after pregnancy.
Ducts. These are channels which take milk from the lobules to the nipple.
Fatty tissue and supporting connective tissue.
Blood vessels, lymph channels and nerves (like all other areas of the body).
Are there different types of breast cancer?
Types of breast cancer
Carcinoma in situ
Some people are diagnosed when the cancerous cells are still totally within a duct or lobule. These are called carcinoma in situ (or non-invasive breast cancer), as no cancer cells have grown out from their original site.
Ductal carcinoma in situ (DCIS) is the most common type of non-invasive breast cancer and about 1 in 5 new breast cancer cases will be DCIS. A carcinoma in situ is easier to treat and has a better outlook than an invasive cancer.
Lobular carcinoma in situ (LCIS) results in abnormal cells in the milk producing glands of the breasts. These cells rarely spread outside of the lobules to other parts of the breast or body.
Invasive breast cancer
Most breast cancers are diagnosed when a tumour has grown from within a duct or lobule into the surrounding breast tissue. These are called invasive breast cancers:
Invasive ductal breast cancers begin in one of the ducts of the breast (see diagram below). They account for as many of 8 in 10 of breast cancer cases.
Invasive lobular breast cancers begins in one of the lobes of the breast. They account for about 1 in 10 of invasive breast cancers.
Invasive breast cancers are also divided into those where cancer cells have invaded into local blood or lymphatic vessels and those that have not. Invasive breast cancer is able to spread outside the breast.
Inflammatory breast cancer
Inflammatory breast cancer is an uncommon form of breast cancer but is very aggressive. It is often very advanced by the time of diagnosis. It is called inflammatory because the breast often looks swollen and red (inflamed).
Inflammatory breast cancer tends to be diagnosed in younger women and because it is aggressive and often diagnosed at a late stage. The outlook is usually worse than for other breast cancers.
Paget's disease of the breast
Paget's disease of the breast is a rare type of cancer of the nipple area of the breast. It presents as eczema affecting the nipple and is often associated with an underlying in-situ or invasive carcinoma of the breast.
Breast cancer symptoms
How do I check for breast cancer myself?
Many women find that their breasts become more lumpy and tender before periods. Breasts also alter their size and shape with increasing age, pregnancy and marked weight changes. What is important is that you get to know your own breasts - how they look and feel - and report any changes promptly to a doctor.
There are a number of things to look out for which might be breast cancer signs:
A breast lump
The usual first sign is a painless lump in the breast. Note: most breast lumps are not cancerous (malignant). Most breast lumps are fluid-filled cysts or fibroadenomas (a clumping of glandular tissue) which are non-cancerous (benign). However, you should always see a doctor if a lump develops, as the breast lump may be cancerous (malignant).
Other signs and symptoms of breast cancer
Other signs which may be noticed in the affected breast include:
Changes in the size or shape of a breast.
Dimpling or thickening of some of the skin on a part of a breast.
The nipple turning in (becoming inverted).
Rarely, a discharge occurring from a nipple (which may be bloodstained).
A rare type of breast cancer, causing a rash around the nipple, which can look similar to a small patch of eczema.
Rarely, pain in a breast. Note: pain is not a usual early symptom. Many women develop painful breasts (mastalgia) and this is not usually caused by cancer.
The first place that breast cancer usually spreads to is the lymph glands (nodes) in the armpit (axilla). If this occurs, you may develop a swelling or lump in an armpit. If the cancer spreads to other parts of the body then various other symptoms can develop.
Breast cancer stages
How many breast cancer stages are there?
Like any other cancer, breast cancer can be divided into stages depending on how much the cancer has spread both within the breast and also to other parts of the body. This helps to decide which treatments are best to use and also helps to give some idea of how likely it is that the breast cancer can be cured.
Breast cancer can be divided into the following stages at the time of diagnosis:
Stage 0
This means that the cancer has not grown away from the original site (for example, a breast duct or milk gland). This is sometimes called 'in situ' (see below).
Stage I
The cancer has spread into fatty breast tissue or a few cancer cells have spread to the glands (lymph nodes) - for example, in your armpit (axilla).
Stage 2
The cancer has either become a bit bigger or many more cancer cells have spread into up to 3 lymph nodes.
Stage 3
The cancer has become more advanced and has spread to the chest wall or the skin around your breast, or has spread to a larger number of lymph nodes.
Stage 4
Breast cancer cells have spread away from the breast and lymph nodes to more distant parts of the body. The most common sites are bones, lungs, liver and brain.
Grade of the cancerous cells
A sample of breast cancer tissue can be looked at under the microscope. By looking at certain features of the cells, the cancer can be graded.
Grade 1 - the cancer cells tend to be slow-growing and less aggressive.
Grade 2 - is a middle grade.
Grade 3 - the cancer cells tend to be fast-growing and more aggressive.
Presence of receptors
Some breast cancer cells have receptors, which allow certain types of hormones or proteins to attach to the cancer cell. The types of receptor tested for are:
Hormones. Tests on a sample of breast cancer cells can show if they contain oestrogen or progesterone receptors. These are female hormones. Overall, about 7 in 10 breast cancers are oestrogen receptor positive. Treatment can block the oestrogen in these cancers (see below).
Human epidermal growth factor (HER2) is a protein that can affect the growth of some cancer cells. It is found on the surface of normal breast cells. Some breast cancer cells have a very high number of HER2 receptors. Cancers having high levels of these receptors are called HER2-positive.
If a sample of cancer cells does not have any oestrogen, progesterone or HER2 receptors, it is called 'triple negative' breast cancer. It affects up to 20% of women with breast cancer and they tend to be a younger age group.
See the separate leaflet called Cancer for more general information about cancer.
Causes of breast cancer
A cancerous (malignant) tumour starts from one abnormal cell. The exact reason why a cell becomes cancerous is unclear. It is thought that something damages or alters certain genes in the cell. This makes the cell abnormal and multiply out of control.
Risk factors
What are the risk factors for breast cancer?
Although breast cancer can develop for no apparent reason, there are certain risk factors which increase the chance that breast cancer will develop. These include:
Age. The risk of developing breast cancer roughly doubles for every 10 years of age. Most cases develop in women over the age of 50.
Where you live. The rate of breast cancer varies between countries. This may reflect genetic or environmental factors.
Family history. This means if you have close relatives who have or have had breast cancer. In particular, if they were aged under 50 when diagnosed.
If you have had a previous breast cancer.
Being childless, or if you had your first child after the age of 30.
Not having breast-fed your children.
Early age of starting periods.
Chest being exposed to radiation.
Having a menopause over the age of 55.
Taking continuous combined hormone replacement therapy (HRT) for several years (in women over 50 years) leads to an increased risk.
Excess alcohol.
Family history and genetic testing
About 1 in 20 cases of breast cancer are caused by a faulty gene which can be inherited. The genes BRCA1 and BRCA2 are the most common faulty genes.
Diagnosing breast cancer
Initial assessment
If you develop a lump or symptoms which may be breast cancer, a doctor will usually examine your breasts and armpits to look for any lumps or other changes. You will normally be referred to a specialist for a breast cancer diagnosis. Sometimes a biopsy of an obvious lump (see below) is arranged, but other tests may be done first, such as:
Mammogram. This is a special X-ray of the breast tissue.
Magnetic resonance imaging (MRI) scan of the breast. This is more commonly performed on younger women, who may have denser breast tissue.
What does breast cancer look like?
Editor’s note
Dr Krishna Vakharia, 16th October 2023
The National Institute for Health and Care Excellence (NICE) has recommended that a person should receive a diagnosis or ruling out of cancer within 28 days of being referred urgently by their GP for suspected cancer.
Biopsy - to confirm the diagnosis
A biopsy is a procedure in which a small sample of tissue is removed from a part of the body. The sample is examined under the microscope, to look for abnormal cells. A specialist may take a biopsy with a needle which is inserted into the lump for some cells to be withdrawn. Sometimes the doctor may be guided as to where to insert the needle with the help of a mammogram or ultrasound scan. Sometimes a small operation is needed to obtain a biopsy sample.
The biopsy sample can confirm or rule out breast cancer. Also the cells from a tumour can be assessed and tested to determine their grade and receptor status (see above).
Assessing the extent and spread
If you are confirmed to have breast cancer, further tests may be needed to assess if it has spread - for example:
An ultrasound scan of the liver.
Chest X-ray.
A bone scan.
Other types of scan.
Playlist: Breast Cancer Spread
2 videos
How far can breast cancer spread?
Dr Sarah Jarvis
How far can breast cancer spread?
Dr. Sarah Jarvis

Can breast cancer spread to the rest of the body?
Dr. Sarah Jarvis
Separate leaflets describe each of these tests in more detail. This assessment is called staging of the cancer. The aim of staging is to find out:
How large the tumour has grown.
Whether the cancer has spread to local lymph nodes in the armpit.
Whether the cancer has spread to other areas of the body (metastasised).
See the separate leaflet called Stages of Cancer for more details.
Finding out the stage of the cancer, the grade of the cells and the receptor status of the cancer helps doctors to advise on the best treatment options. It also gives a reasonable indication of outlook.
How often is breast cancer misdiagnosed?
Breast cancer treatment
What is the best treatment for breast cancer?
Treatment options which may be considered include surgery, chemotherapy, radiotherapy and hormone treatment. Often a combination of two or more of these treatments is used. The treatments used depend on:
The cancer itself - its size and stage (whether it has spread), the grade of the cancer cells, and whether it is hormone responsive or contains HER2 receptors; AND
The woman with the cancer - your age, whether or not you have had your menopause, your general health and personal preferences for treatment.
You should have a full discussion with a specialist who knows your case. They will be able to give the pros and cons, likely success rate, possible side-effects and other details about the various possible treatment options for your type of cancer.
You should also discuss with your specialist the aims of treatment. For example:
Treatment aims to cure the cancer in many cases. In particular, the earlier the stage of the cancer, the better the chance of a cure. Because of routine mammography, many women are diagnosed with breast cancer in the early stages and have a good chance of a cure. Doctors tend to use the word remission rather than the word cured. Remission means there is no evidence of cancer following treatment. If you are in remission, you may be cured. However, in some cases a cancer returns months or years later. This is why doctors are sometimes reluctant to use the word cured.
Treatment may aim to control the cancer. If a cure is not realistic, with treatment it is often possible to limit the growth or spread of the cancer so it progresses less rapidly. This may keep you free of symptoms for some time.
Treatment may aim to ease symptoms of breast cancer in some cases. Even if a cure is not possible, treatments may be used to reduce the size of a tumour, which may ease symptoms such as pain. If a cancer is advanced then you may require treatments such as nutritional supplements, painkillers, or other techniques to help keep you free of pain or other symptoms.
Surgery for breast cancer
The types of operation which may be considered are:
Breast-conserving surgery. This is often an option if the tumour is not too big. A lumpectomy (or wide local excision) is one type of operation where just the tumour and some surrounding breast tissue are removed. It is usual to have radiotherapy following this operation. This aims to kill any cancer cells which may have been left in the breast tissue.
Removal of the affected breast (mastectomy). This may be necessary if there is a large tumour or a tumour in the middle of the breast. It is often possible to have breast reconstructive surgery to create a new breast following a mastectomy. This can often be done at the same time as the mastectomy, although it can also be done months or years later. There are now many different types of reconstruction operations available.
A sentinel lymph node biopsy may be performed. This is a way of assessing if the main lymph nodes draining the breast contain cancer. If they are clear then the remaining lymph nodes in the armpit will not need to be removed. If it is not possible to do this, one or more of the lymph nodes in the armpit may be removed. This helps to stage the disease accurately and to guide the specialist as to what treatment to advise following surgery.
Radiotherapy
Radiotherapy is a treatment which uses high-energy beams of radiation which are focused on cancerous (malignant) tissue. This kills cancer cells, or stops cancer cells from multiplying. See the separate leaflet called Radiotherapy for more details.
For breast cancer, radiotherapy is mainly used in addition to surgery. For example, if you have breast-conserving surgery it is usual to have radiotherapy to the affected breast after the operation. This aims to prevent breast cancer returning in the same breast. When radiotherapy is used in addition to surgery it is called adjuvant radiotherapy.
Hormone treatments
Some types of breast cancer are affected by the female hormones oestrogen and progesterone. These hormones stimulate the cancer cells to divide and multiply. Most oestrogen and progesterone are made by the ovaries. Treatments which reduce the level of these hormones, or prevent them from working, are commonly used in people with breast cancer.
Hormone treatment works best in women with hormone-responsive breast cancer; however, it sometimes works in cancers classed as non-hormone-responsive.
Hormone treatments include:
Oestrogen blockers. Tamoxifen has been available for many years and is still widely used. It works by blocking the oestrogen from working on cells. It is usually taken for five years. Other oestrogen blocker medicines are now available.
Aromatase inhibitors. These are medicines which work by blocking the production of oestrogen in body tissues. They are used in women who have gone through the menopause. These medicines include anastrozole, letrozole and exemestane.
Gonadotrophin-releasing hormone (GnRH) analogues. These medicines work by greatly reducing the amount of oestrogen that you make in the ovaries. There are several GnRH analogue preparations. The commonly used one is goserelin. They are usually given by injection and may be used for women who have not yet reached the menopause.
An alternative which may be considered for women before the menopause is to remove the ovaries (or to destroy them with radiotherapy). This stops oestrogen from being made.
Chemotherapy
Chemotherapy is a treatment of cancer by using anti-cancer medicines which kill cancer cells, or stop them from multiplying. See the separate leaflet called Chemotherapy for more details.
When chemotherapy is used in addition to surgery it is known as adjuvant chemotherapy. For example, following surgery you may be given a course of chemotherapy. This aims to kill any cancer cells which may have spread from the main tumour site.
Chemotherapy is sometimes given to shrink a tumour before surgery so that surgery may have a better chance of success and also a smaller operation may be performed. This is known as neoadjuvant chemotherapy. The type of chemotherapy given may depend on the type of cancer.
New gene tests are being developed to help doctors decide which women will benefit the most from chemotherapy - see Further Reading.
Chemotherapy may also be used for some women to treat breast cancer which has spread to other areas of the body.
Trastuzumab (also known as Herceptin®) is a treatment that may be given to women who have a large number of HER2 receptors in their cancer. It is a type of medicine called a monoclonal antibody. It works by attaching to HER2 receptors on the surface of breast cancer cells, thereby stopping the cancer cells from dividing and growing.
Editor’s note
Dr Krishna Vakharia, 15th December 2022
NICE has advised that pembrolizumab is an option for adults with triple-negative early breast cancer at high risk of recurrence or in locally advanced breast cancer.
It has been shown that by adding pembrolizumab to chemotherapy before surgery (neoadjuvant) and then continuing with pembrolizumab alone after surgery (adjuvant), there is an increased chance the cancer will disappear. It also increases the time before any cancer comes back again.
Dr Krishna Vakharia, 22nd February 2023
NICE has recommended the option of trastuzumab deruxtecan with managed access for treating HER2-positive unresectable or metastatic breast cancer but only after they have had one or more anti-HER2 treatments.
Managed access means that this medication is only available to certain people as there is not much evidence for its use. Whilst people take it, information is collected and analysed to see whether it should be available to all who need it on the NHS. This process allows people access to promising new medications and treatments whilst gathering evidence.
In the case of trastuzumab deruxtecan, we know that it delays the time in which someone's cancer gets worse but we don't know yet if it allows people to live longer.
In summary
The treatment plan that may be advised can vary greatly from case to case as optimal treatment can depend on many different factors.
What is the prognosis?
What is the breast cancer survival rate?
The outlook (prognosis) has greatly improved in recent years. Deaths from breast cancer are now at the lowest ever in 40 years. This is mainly due to the improvements in the treatment of breast cancer. The outlook is best in those who are diagnosed when the cancer is still small and has not spread. More breast cancers are also now being diagnosed and treated at an early stage. In general, the more advanced the cancer (the more it has spread) then the less chance that treatment will be curative.
The treatment of cancer is a developing area of medicine. New treatments continue to be developed and the information on outlook above is very general. The specialist who knows your case can give more accurate information about your particular outlook and how well your type and stage of cancer is likely to respond to treatment.
Screening for breast cancer
Women in the UK aged between 50 and 70 are invited to have a routine mammography every three years. This is gradually being extended to women aged 47-73.
Mammography is a special X-ray test and aims to detect breast cancer at an early stage when treatment is most likely to be curative. See the separate leaflet called Breast Screening.
Genetic testing and mammography screening (and preventative treatments in some cases) may also be offered to younger women with a strong family history of breast cancer. See your doctor if you feel this applies to you.
Is breast cancer genetic?
Can breast cancer be prevented?
A lot of breast cancers are detected at an early stage, by breast screening. However, a small number are not. Some women may have developed breast cancer before they have their first mammogram and some may develop breast cancer between mammograms.
All women of every age should be breast aware. That is, get to know how your breasts and nipples normally look and feel. Try to recognise any changes that occur before and after your periods. See your GP if you notice any changes, lumps, or other abnormalities in your breasts or nipples. Don't wait until your next scheduled screening appointment.
There is some evidence that regular exercise may reduce your risk of breast cancer by as much as a third. If you have been through the menopause, it is particularly important you are not overweight or obese. This is because being overweight causes more oestrogen to be produced, which can increase the risk of breast cancer.
Studies have shown that women who breast-feed their children are less likely to develop breast cancer than those who do not. The most likely reason for this is that women do not produce an egg (ovulate) as regularly while they are breast-feeding and oestrogen levels remain stable.
A further study also suggests that switching from red meat to white meat may also reduce the risk of developing breast cancer by more than a quarter.
There is also preventative surgery to remove the breasts (mastectomy). Surgery can be used to treat breast cancer as well as reduce the chances of developing it. By removing as much breast tissue as possible, a mastectomy can reduce your risk of breast cancer by up to 90%. Like all operations there can be several complications and this is not an easy step to take. If genetic testing has shown you are one of the small number of women from a high-risk family, you will need an in-depth discussion with your doctors, before deciding to have this operation.
Medicines which reduce the levels of oestrogen in the body are also used. They have significant side-effects (like hot flushes and reducing bone strength). Your specialist will discuss the risks and benefits of these options with you.
Patient picks for Breast cancer

Cancer
Mammogram
A mammogram is a low-dose X-ray used to check breasts for cancer. In the UK, women aged 50 to 70 years are invited every three years for a mammogram as part of the breast screening service. Mammograms are also used in breast clinics if a breast lump needs checking.
by Dr Philippa Vincent, MRCGP

Cancer
BRCA genes
There are a few known gene changes (mutations) that can increase the risk of certain cancers, and tests available for some of them, including BRCA1 and BRCA2 gene mutations. The BRCA1 and BRCA2 genes normally protect against certain cancers, particularly breast cancer and ovarian cancer. If there is a mutation in one of these genes then this may mean that the protection is lost and that a cancer is more likely to develop.
by Dr Colin Tidy, MRCGP
Frequently asked questions
Can men get breast cancer?
Yes, breast cancer can also develop in men, though it is considerably less common than in women.
What is the difference between ductal carcinoma in situ (DCIS) and invasive ductal breast cancer?
Ductal carcinoma in situ (DCIS) means that the cancerous cells are entirely contained within the milk ducts and have not spread beyond their original site. Invasive ductal breast cancer, on the other hand, means the tumor has grown from within a duct into the surrounding breast tissue.
What is a 'triple negative' breast cancer?
Triple negative breast cancer is when the cancer cells do not have oestrogen receptors, progesterone receptors, or HER2 receptors. This type affects up to 20% of women with breast cancer and is often found in a younger age group.
How do doctors determine the 'grade' of breast cancer?
A sample of breast cancer tissue is examined under a microscope to look at specific features of the cells. Based on these features, the cancer is graded, with Grade 1 cells being slow-growing and less aggressive, Grade 2 being a middle grade, and Grade 3 cells being fast-growing and more aggressive.
What kinds of changes to my nipple should I be concerned about?
You should be concerned about changes such as the nipple turning inward (becoming inverted), or a discharge from the nipple, especially if it is bloodstained. Additionally, a rash around the nipple that looks similar to eczema could be a sign of a rare type of breast cancer, called Paget's disease. Any of these changes should be reported to a doctor promptly.
What is the purpose of hormone treatments for breast cancer, and when are they used?
Hormone treatments are used for breast cancers that are affected by female hormones like oestrogen. These treatments either reduce the levels of these hormones or prevent them from working to slow down or stop the growth of cancer cells. They are most effective in women with hormone-responsive breast cancer, but sometimes work even in non-hormone-responsive cases. Different types of hormone treatments are available, depending on a woman's menopausal status.
Further reading and references
- Breast cancer statistics; Cancer Research UK
- Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer; NICE Clinical Guideline (June 2013 - last updated November 2023).
- Advanced breast cancer: Diagnosis and treatment; NICE Clinical Guideline (July 2014, updated Aug 2017)
- Suspected cancer: recognition and referral; NICE guideline (2015 - last updated April 2026)
- Breast cancer - recognition and referral; NICE CKS April 2025 (UK access only)
- Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer; Sparano JA et al, New England Journal of Medicine, June 2018
- Early and locally advanced breast cancer: diagnosis and management; NICE Guideline (July 2018 - last updated April 2025).
- Welslau M, Muller V, Luftner D, et al; Update Breast Cancer 2022 Part 1 - Early Stage Breast Cancer. Geburtshilfe Frauenheilkd. 2022 Jun 3;82(6):580-589. doi: 10.1055/a-1811-6106. eCollection 2022 Jun.
- Pembrolizumab for neoadjuvant and adjuvant treatment of triple-negative early or locally advanced breast cancer; NICE Technology appraisal guidance, 14 December 2022
- Trastuzumab deruxtecan for treating HER2-positive unresectable or metastatic breast cancer after 1 or more anti-HER2 treatments; NICE Technology appraisal guidance, February 2023
About the authorView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
About the reviewerView full bio

Dr Rosalyn Adleman, MRCGP
MRCGP
Dr Rosalyn Adleman, is an NHS GP working in north London.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 13 Oct 2027
31 Oct 2022 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in cancer
- Acute myeloid leukaemia
- BRCA genes
- Breast screening
- Cancer
- Cancer of the uterus
- Cancer treatment
- Cervical screening
- Children's cancers
- Chronic lymphocytic leukaemia
- Chronic myeloid leukaemia
- Gynaecological cancer
- Lung cancer
- Mammogram
- Mouth cancer
- Mucositis
- Non-melanoma skin cancer
- Paget's disease of bone
- Preventing skin cancer
- Retinoblastoma
- Testicular cancer