Kawasaki disease
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 13 Nov 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Kawasaki disease is a rare condition that affects small to medium-sized blood vessels in the body. Kawasaki disease causes the the walls of the blood vessels to become inflamed and swollen (vasculitis). Kawasaki disease mainly affects children less than 5 years old. The exact cause of Kawasaki disease remains unknown. Kawasaki disease causes a high temperature (fever), a rash, and other typical symptoms (listed below).
The most serious complication of Kawasaki disease occurs when the arteries supplying the heart (coronary arteries) are affected. This occurs in about 1 in 4 children with untreated Kawasaki disease. Treatment with intravenous immunoglobulin and aspirin has greatly reduced the proportion of children with Kawasaki disease who develop coronary artery problems.
The outcome for children diagnosed with Kawasaki disease is mainly based on the extent and severity of coronary artery involvement. Kawasaki disease is fatal in less than 1 in 500 of those affected.
At a glance
Kawasaki disease is an uncommon condition mainly affecting children under 5 years old.
It causes a high temperature for at least five days, with various other symptoms throughout the body.
There is no specific test; diagnosis relies on typical symptoms.
The cause is unknown, but it is not contagious.
Without treatment, up to 1 in 4 children may develop heart complications.
Treatment with immunoglobulin and aspirin reduces the risk of heart complications.
See a doctor if your child has a fever for five days or more.
What is Kawasaki disease and who gets it?
It is an uncommon condition that mainly affects children aged under 5 years. It most commonly affects children aged 18-24 months. It causes various symptoms throughout the body (listed below). Kawasaki disease was first described in the 1960s by a Japanese doctor named Tomisaku Kawasaki. Since then cases have been reported in many countries.
Kawasaki disease is also occasionally known as mucocutaneous lymph node syndrome.
It is much more common in some countries than it is in others. It seems to be particularly common in Japan. It is less common in Europe and the USA. It affects boys more often than it affects girls. It seems to run in families. So it is more common in siblings or children of people who have had the disease in the past.
Kawasaki disease symptoms
A high temperature (fever) which lasts at least five days is usual. If your child has a fever for five days or more, you should see your doctor, who should assess them to see if they might have Kawasaki disease. In addition, at least four of the following normally develop:
Bloodshot eyes
Redness of the eyes (conjunctivitis) without sticky discharge.
Strawberry tongue
Changes in the mouth such as a red throat or tongue, or dry and cracked lips.
Strawberry tongue
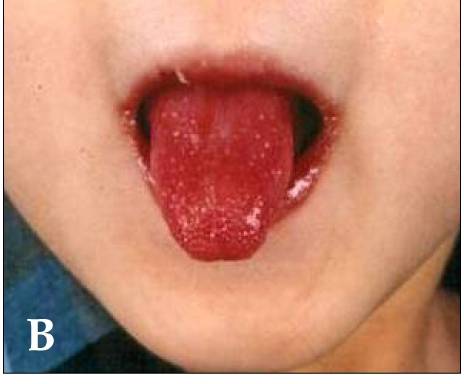
© Kawasaki_symptoms.jpg: Dong Soo Kimderivative work: Natr, CC BY 2.0, via Wikimedia Commons
Kawasaki rash
A rash. This normally fades within a week. There is no specific 'Kawasaki rash' - the appearance may be different in different children. Most often there are raised red blotchy areas. It tends to affect a lot of the body, particularly the chest, tummy, back, groins, hands and feet.
Peeling of fingers
Changes in the hands or feet such as mild swelling or redness. The skin on some of the fingers or toes often peels after about 2-3 weeks.
Swollen lymph glands
One or more lymph glands in the neck become swollen.
It's important to remember that some of these symptoms may settle. That means you need to tell your doctor if your child has had any of these symptoms, even if they have gone away on their own.
Children under 1 year old may not have as many other features of Kawasaki disease apart from fever. However, it is very important that they are checked out and referred for tests if the doctor thinks they may have Kawasaki disease.
Also, affected children are commonly very irritable. The diagnosis is based on the above typical group of symptoms. There is no test to confirm the disease. Tests may be done to rule out other diseases that cause similar symptoms, such as measles, scarlet fever, etc.
Other symptoms may develop in addition to the above. These are less common and include:
Diarrhoea.
Being sick (vomiting).
Tummy (abdominal) pains.
Being off food.
Joint swelling and pains.
Skin going yellow (jaundice).
Typically, fever develops first and then the other symptoms (listed above) develop after a few days. Often, the symptoms that develop after the high temperature (fever) has started develop one after each other rather than all coming on at the same time. This is why the diagnosis may take several days to make after the initial fever starts. In total, symptoms tend to last up to 10 days before easing and going, although complications sometimes develop (see below).
During the illness, some children become very unwell, but others have a mild illness. This may be similar to many common infections that are caused by a virus. However, any child suspected of having Kawasaki disease is normally admitted to hospital, even if they appear to have a mild illness.
What causes Kawasaki disease?
The cause is not known. The symptoms seem rather like many common infections. However, it is not catching (contagious). It is rare for contacts of affected children also to become affected at the same time. This means that the cause is unlikely to be just an infection with a germ such as a bacterium or virus. It may be an unusual or severe reaction to a common virus that usually causes little or no harm to most people. However, no virus or other germ has been proved to cause this disease.
There seems to be some genetic tendency that increases the risk of developing the condition. For example, parents of children with Kawasaki disease are more likely to have had the condition themselves during childhood. Also, brothers and sisters have an increased risk of developing the condition. So, a theory is that affected children may have a genetic make-up that makes them 'overreact' to a common viral infection that does not cause problems in most children.
Kawasaki disease diagnosis
There is no specific test. So it is usually diagnosed on the basis of the typical features. Blood tests may point towards the diagnosis, or be used to rule out other possible diagnoses.
A heart scan (echocardiogram, or echo) is normally done to look for complications (see below). If complications do occur, they usually develop a week or so after the symptoms listed above. If heart complications occur, other types of scans may be used to monitor these over time.
Kawasaki disease treatment
Aspirin. This is one of the few times aspirin is given to children. Aspirin helps to reduce the inflammation in the coronary arteries. It also helps to prevent clots in the blood. The flu jab (influenza vaccination) is usually given to children who have had aspirin treatment if they have not yet had their annual vaccination. This prevents some of the complications which can be caused by aspirin in children.
Immunoglobulin. This is an antibody mixture obtained from human blood. It is given by a slow injection over a few hours (infusion) into the bloodstream. You may see it referred to as IVIg - intravenous immunoglobulin. It is not clear how it works. It may modify the response of the immune system in some way to prevent inflammation in the arteries.
Treatment with immunoglobulin given within 10 days of the onset reduces the chance of heart complications (see below). Without treatment, about 25 in 100 affected children develop an aneurysm. With treatment, this is reduced to fewer than 5 in 100. In some cases the immunoglobulin treatment is not effective and other options are tried.
Other treatments aim to make the child comfortable, such as giving lots to drink and nursing them through the acute feverish illness.
Research continues to search for better treatments. Some treatments which have been tried or are being studied are:
Further research is needed to confirm the role of these medicines in the treatment of Kawasaki disease.
If aneurysms have developed (see complications section below), a specialist heart doctor for children (a paediatric cardiologist) will be involved. In this situation, treatment is needed to prevent heart attacks or other heart problems developing. The child will have regular heart scans to keep an eye on what is happening. He or she may need another medicine to stop a blood clot. Very occasionally an operation is needed on the heart.
Some vaccines - particularly measles, mumps and rubella (MMR) - may need to be delayed for some months after IVIg treatment, which may cause them to be less effective.
Complications
Heart problems
Without treatment, up to 1 in 4 children who have Kawasaki disease develop inflammation of the blood vessels to the heart (coronary arteries). This can cause a swelling of a section of a coronary artery, which is called an aneurysm.
A coronary artery aneurysm usually causes no symptoms. Over time it often goes away and the artery returns to normal. However, the wall of an aneurysm is weakened and abnormal. Serious problems may develop in some children with an aneurysm. The most serious is that a clot (thrombosis) may develop in the aneurysm. The muscle of the heart is supplied with oxygen, carried in the blood of these arteries. If a clot develops, the muscle does not get enough oxygen. The heart muscle can then be damaged, causing a heart attack. Currently fewer than 1 in 100 children with Kawasaki disease die of heart problems.
An aneurysm can be detected by a heart scan (an echocardiogram, or echo). If an aneurysm does occur, it starts to develop a week or more after the fever and other acute symptoms begin. Treatment within 10 days of symptoms starting often prevents an aneurysm developing.
Other complications
The aneurysm of a coronary artery is caused by inflammation of the artery (a 'vasculitis'). This swelling can occur in other arteries in various parts of the body, causing aneurysms elsewhere - but this is very rare. Various other rare problems have also been reported in some children with Kawasaki disease.
Kawasaki disease in adults
Kawasaki disease usually affects children. However in rare cases, it can occur in adults. Also, children who have had heart complications due to Kawasaki disease may continue to be affected by these when they reach adulthood. For example, women who had Kawasaki disease as children may not be able to have certain contraceptive pills, and may need specialist advice about whether it is safe for them to become pregnant.
Patient picks for General health conditions

Children's health
Eczema in children
Most children with eczema have atopic eczema, but some children with eczema have a different condition called contact dermatitis - which is a reaction to a substance on or near the skin. It is not unusual for a child with atopic eczema to also have contact dermatitis to certain products applied to the skin. There are other types of eczema, which are much less common in children.
by Dr Colin Tidy, MRCGP

Children's health
Back pain in children
Back pain in children occurs quite often and seems to be increasingly common. Most of the time this is not a serious problem.
by Dr Toni Hazell, FRCGP
Frequently asked questions
Why is delayed treatment for Kawasaki disease within 10 days so important?
Receiving treatment, particularly with immunoglobulin, within 10 days of the start of symptoms significantly reduces the chance of developing heart complications, such as an aneurysm in the coronary arteries. Without treatment, about 25 in 100 affected children develop an aneurysm, but with timely treatment, this is reduced to fewer than 5 in 100.
What happens if an aneurysm develops in the heart due to Kawasaki disease?
If an aneurysm develops in a coronary artery, it usually doesn't cause symptoms initially and often resolves on its own over time. However, the weakened and abnormal artery wall can lead to serious problems, most notably a blood clot forming within the aneurysm. This clot can restrict blood flow to the heart muscle, potentially causing damage and a heart attack. If an aneurysm is detected, a paediatric cardiologist will be involved to manage the condition, which may include regular heart scans and medication to prevent blood clots. In very rare cases, heart surgery might be necessary.
Can Kawasaki disease be caught from other people?
No, Kawasaki disease is not contagious. It is rare for people in close contact with an affected child to also develop the disease. While the symptoms resemble common infections, the cause is not directly from a germ like a bacterium or virus that can be passed from person to person.
What is mucocutaneous lymph node syndrome?
Mucocutaneous lymph node syndrome is another name occasionally used for Kawasaki disease. It refers to the involvement of mucous membranes (like in the mouth and eyes) and lymph nodes, which are characteristic symptoms of the condition.
What other treatments might be considered if initial treatment with immunoglobulin isn't effective?
If immunoglobulin treatment is not effective, other options that have been tried or are currently being studied include steroids like prednisolone, infliximab, etanercept, and methotrexate. However, further research is needed to confirm the role of these medicines in treating Kawasaki disease.
What is the typical time frame for Kawasaki disease symptoms to last?
Typically, the symptoms of Kawasaki disease tend to last for up to 10 days before they begin to ease and resolve. However, complications can sometimes develop after this initial period.
Further reading and references
- Owens AM, Plewa MC; Kawasaki Disease. StatPearls, Jan 2024.
- Kuo HC; Diagnosis, Progress, and Treatment Update of Kawasaki Disease. Int J Mol Sci. 2023 Sep 11;24(18):13948. doi: 10.3390/ijms241813948.
- Rife E, Gedalia A; Kawasaki Disease: an Update. Curr Rheumatol Rep. 2020 Sep 13;22(10):75. doi: 10.1007/s11926-020-00941-4.
- Green J, Wardle AJ, Tulloh RM; Corticosteroids for the treatment of Kawasaki disease in children. Cochrane Database Syst Rev. 2022 May 27;5(5):CD011188. doi: 10.1002/14651858.CD011188.pub3.
- Fever in under 5s: assessment and initial management; NICE Guidance (last updated November 2021)
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 12 Nov 2027
13 Nov 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in children's health
- BCG immunisation
- Bedwetting reward systems
- Breastfeeding your baby
- Cerebral palsy
- Childhood obesity
- Coughs and colds in children
- Dyspraxia
- Head lice and nits
- Left-side abdominal pain in children
- Neonatal jaundice
- Oral thrush in babies
- Pneumococcal immunisation
- Respiratory syncytial virus (RSV)
- Rubella
- Safeguarding children
- Symptoms of sepsis in children
- Toddler's diarrhoea
- Wilson's disease