Turner syndrome
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 22 Feb 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Turner syndrome is a genetic condition that only affects girls. The most characteristic features of the syndrome are being short, having certain physical features (detailed below), and ovaries that do not work properly. Although there is no cure, there are treatments that can help most girls with Turner syndrome lead relatively normal lives.
At a glance
Turner syndrome is a genetic condition affecting only females from conception.
It occurs when a female has only one complete X chromosome, instead of two.
Features can include short stature, distinct facial features, and bone differences.
Medical symptoms can include susceptibility to certain conditions and organ abnormalities.
Diagnosis is confirmed by a karyotype test, which examines chromosomes.
Treatments can help manage aspects like growth and hormone levels.
Life expectancy is usually only slightly reduced, and quality of life is often normal.
What is Turner syndrome?
Turner syndrome (TS) only occurs in females and is present from the time of conception. It describes a set of features which occur when a female has only one complete X chromosome in each cell. The second X chromosome may be missing entirely or may be incomplete. See below to read more about chromosomes and the abnormality present in Turner syndrome.
Can Turner syndrome be inherited?
Turner syndrome is a genetic condition. This means that there is an abnormality with the genes of the affected person. Genes are passed on to a child from each parent, in structures called chromosomes.
You have 23 pairs of chromosomes in each cell of your body. That is, a total of 46 chromosomes. Each chromosome contains thousands of genes. Our genes determine how our body functions, what we look like and sometimes what diseases we will get. The genes that control which sex (gender) we become are part of the chromosomes called sex chromosomes. These can be either X or Y chromosomes. We get one sex chromosome from each parent.
Usually, a female has two copies of the X chromosome and a male has one X and one Y chromosome. An individual's complete set of chromosomes is known as their karyotype. So the karyotype of most women is said to be 46,XX and the karyotype of most men is said to be 46,XY.
Turner syndrome chromosomes
Girls and women with Turner syndrome have only one X chromosome. The karyotype is therefore said to be 45,X or 45,XO.
How common is Turner syndrome?
Turner syndrome occurs in about one in 2,000 live female births. There are no known risk factors for Turner syndrome. It is not more common in girls born to older women and it is very rare to have a second child with Turner syndrome.
Turner syndrome features
Turner syndrome features that may develop before birth are thickness of the neck tissue, a neck swelling called a cystic hygroma, or being a small-sized baby.
Newborn babies with Turner syndrome may have lymphoedema of the hands and feet and excess skin of the neck.
As girls become older, a range offeatures may develop. The following are some of the more common:
Short stature
Most girls with Turner syndrome will be short for their age.
Typical facial features
This may include characteristic changes to the eyes, ears, mouth and neck - for example:
Downslanting eyes.
Droopy eyelids.
Prominent earlobes.
Crowding of the teeth.
A short webbed-like neck.
Bone features
For example:
A broad chest with widely spaced nipples.
A wide carrying angle (this is the angle between the forearm and the hip when the arm is held by the side).
Short fingers.
Nail changes.
Skin features
Girls with Turner syndrome often have a lot of moles and obvious blood vessels over the skin.
Turner syndrome symptoms
The medical symptoms of Turner syndrome will vary depending on the age of the girl or woman.
Before a girl with Turner syndrome is born, she may have a problem called lymphoedema. This occurs when fluid is not able to be transported around the body and organs properly. So, some fluid leaks into tissues and causes swelling.
The following symptoms can occur in Turner syndrome:
Susceptibility to certain medical conditions
People with Turner syndrome are more likely to develop certain conditions such as:
Organ abnormalities
For example, about half will have an abnormality with the heart or major blood vessels. Up to 6 in 10 will have an abnormality of the kidneys or urinary tract.
Ovarian abnormalities
The ovaries are a pair of glands that lie on either side of the womb (uterus). Each ovary is about the size of a large marble. The ovaries normally make eggs (ova) and various female hormones - in particular, oestrogen. Almost all girls with Turner syndrome have ovaries that do not work properly. As a result, they
May not go through puberty.
May have breasts which do not develop properly.
May not ever get a period, and are likely to be infertile. However, up to 3 in 10 girls will have some changes of puberty and 1 in 200 may be able to get pregnant naturally.
Note: although there are often problems with ovaries, women with Turner syndrome still have a normal vagina and womb and can have a normal sex life.
What does Turner syndrome look like?
Turner syndrome
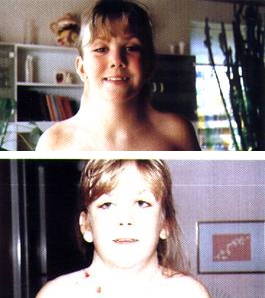
© Johannes Nielsen (own work),via Wikimedia Commons
Turner syndrome complications
Turner syndrome may lead to the development of secondary abnormalities. The most common are as follows:
Heart and blood vessel complications.
Heart valves may become faulty, abnormalities on the heart tracing (electrocardiogram, or ECG), or abnormalities of the main blood vessels such as the main artery that takes blood from the heart (may develop an aneurysm of the aorta). In some cases the aorta can rupture.
High blood pressure is also quite common in Turner syndrome.
Urinary abnormalities
Extra tubes from the kidney to the bladder, only one kidney developing, or unusually shaped kidneys. These abnormalities can make urinary tract infections (urine infections) occur more commonly than usual.
Eye problems
About 8 in 100 girls with Turner syndrome have colour vision problems and may develop poor vision over time.
Ear problems
Hearing impairment is common and can be due to persistent (chronic) ear infections or deterioration of the nerves.
'Thinning' of the bones
This is also known as osteoporosis. It may occur later in life as a complication of a lack of oestrogen if oestrogen treatment is not started early enough or taken continuously.
Secondary conditions
About 1 in 4 girls with Turner syndrome develop thyroid problems. A small number develop coeliac disease, which is a problem with the gut due to an intolerance to gluten.
How is Turner syndrome diagnosed?
Turner syndrome may be suspected by your doctor if a girl has some of the above features. The diagnosis can be confirmed by a test called karyotype testing. This involves a sample being taken either from the amniotic fluid around a baby in the womb (uterus), or from a blood sample in children.
The chromosomes can be studied from the sample. When the chromosomes are studied, if there is one X chromosome missing or if it is incomplete in certain parts, this confirms the diagnosis of Turner syndrome.
Can Turner syndrome be detected before birth?
Turner syndrome can be diagnosed before a baby is born, using a test called amniocentesis. Turner syndrome may also be suspected during pregnancy on a routine ultrasound scan if the scan shows any problems with the heart or kidney that are typical of Turner syndrome.
How to test for Turner syndrome
Because there are a number of possible complications of Turner syndrome, certain tests are usually done to diagnose Turner syndrome. Some other tests are then done on a regular basis, sometimes yearly for the rest of your life. The tests include the following:
Blood tests
These include a yearly check of thyroid function, liver function, cholesterol and glucose levels. Every 2-4 years, a blood test for coeliac disease is also advised. A blood test for female hormones may also be done to assess whether the ovaries are working or not.
Hearing assessment
A hearing assessment needs to be done at diagnosis and then every 1-5 years depending on the detection of any hearing loss. If frequent ear infections develop, a specialist review and further treatment may be needed.
Vision testing
This needs to be done at least at the time of diagnosis or at age 1 year, whichever is later, and then repeated as required depending on the issues involved.
Heart check
This is usually done by a heart specialist (cardiologist) and includes tests such as an ultrasound of the heart (echocardiogram), blood pressure check, tracing of the electrical activity of the heart (electrocardiogram, or ECG) and MRI scan of the heart. Some of these tests will need to be done regularly and some will only be required a few times.
It is also very important to have regular monitoring of the size of the aorta, which is the main blood vessel in the body. In some girls with Turner syndrome, this blood vessel becomes wider over time and can burst suddenly (rupture) which may be life-threatening. If the size of the main artery that takes blood from the heart (the aorta) is monitored, appropriate treatment, including surgery, can be given to prevent the aorta from bursting.
Kidney check
An ultrasound scan of the kidneys is usually done when Turner syndrome is diagnosed, to assess for abnormalities with the kidneys and urinary tract.
Bone assessments
For young children with Turner syndrome this will mean testing by the doctor for hip dislocations. Teenagers need to be assessed for a curvature of the spine (scoliosis). Bone density scans to check for osteoporosis are also advised.
Weight and exercise
Encourage children with Turner syndrome to eat healthily and exercise regularly in order to keep weight in the healthy range. This is important because of the increased risk of diabetes and heart problems in Turner syndrome which are more common in overweight people.
Dental check
Due to the small size of the mouth in some girls with Turner syndrome, regular dental checks are advised to manage problems with tooth abnormalities. The most common is a problem with dental occlusion - that is, the way the teeth meet when they bite together.
Turner syndrome treatments
As this is a condition caused by abnormal genes, there is no cure for it.
There are several effective treatments for different aspects of the syndrome which aim to minimise the impact of the condition. These can be divided into medication treatments (such as hormonal therapy) and non-medication treatments (such as psychological therapy).
Medication treatments
The most important medication treatments are:
Growth hormone
This is sometimes started as early as 12-24 months of age. It should definitely be started as soon as it is clear that a child is not growing normally due to Turner syndrome.
Growth hormone replacement therapy has been shown to increase the final height by as much as 10 cm.
Growth hormone therapy is generally continued until a child reaches a bone age of 14. This means that her bones are the same as the bones of a child without Turner syndrome at age 14.
Oestrogen and progesterone
A blood test for these female hormones can indicate if the ovaries are not working and are not producing enough oestrogen. Oestrogen can be given as a tablet, patch or injection. In this type of hormone replacement therapy, the dose is gradually increased over a few years until a dose is obtained that will give normal oestrogen levels.
Progestogen is added later than oestrogen to help to produce withdrawal bleeds (like periods). These hormone treatments are usually continued throughout life.
Non-medication treatments
Various treatments may be needed and include the following:
Psychological therapy
This can be important for a number of girls and women with Turner syndrome. For example, they may have low self-esteem due to their appearance, or their social functioning or because they are infertile.
Sex education
A small number of girls with Turner syndrome will be able to get pregnant naturally. So, if you have Turner syndrome and are sexually active, as with any other female, you need to be informed about contraception and safe sex practices.
Infertility
While a small number of women with Turner syndrome will be able to get pregnant naturally, the vast majority will be infertile. Assisted conception using various forms of IVF may be successful. Regular heart checks before and during pregnancy are essential, as pregnancy increases the strain on the heart and blood vessels.
Learning difficulties
A few girls with Turner syndrome also have learning problems and so specialised assistance with schooling can help to manage this. However, most girls with Turner syndrome have normal intelligence.
Management of lymphoedema
Physiotherapy and support stockings can help to reduce the swelling experienced by some girls with Turner syndrome.
Adults with Turner syndrome
When they become adults, most girls with Turner syndrome will be shorter than average and infertile. However, the development of growth hormone treatment has improved the expected adult height for those treated. The most significant risk faced is that of heart and blood vessel problems. But, regular checks and treatment where necessary have reduced the impact of these complications. Overall:
Life expectancy is only slightly reduced and quality of life is usually normal.
Most girls with Turner syndrome have normal intelligence.
Most have the potential to lead happy and full lives.
Can a woman with Turner syndrome get pregnant?
As above, many women with Turner syndrome will be unable to become pregnant naturally. A small number may do so, however, and others may be able to become pregnant with treatments such as in vitro fertilisation (IVF). However, this should be discussed at length with a specialist doctor, because pregnancy may be more risky for women with Turner syndrome.
This is due to the susceptibility to other medical problems - for example, heart defects. When the heart is put under more pressure due to pregnancy, it can be dangerous. Each woman should be screened for their individual risks, so they can weigh up the pros and cons of pregnancy. This needs specialist help and expertise.
Patient picks for Genetic conditions
Children's health
Congenital pulmonary airway malformation
Congenital pulmonary airway malformation (CPAM) is a rare abnormality of lung development. It is found either in unborn babies or in young babies. The name has recently changed from congenital cystic adenomatoid malformation (CCAM). It is increasingly detected by the routine ultrasound scan during pregnancy. Congenital means present from birth. Pulmonary means related to the lungs. The severity of the abnormality is very variable. Some lesions can shrink or even disappear without treatment. Some lesions cause the baby to have breathing problems very soon after birth. Some lesions cause severe problems for the baby and may have a poor outcome.
by Dr Hayley Willacy, FRCGP

Children's health
Congenital heart disease
Congenital heart disease is a condition where an abnormality (defect) develops in the heart before birth. There are a number of types of congenital heart defect. Some are mild and cause few problems; others are life-threatening for the baby.
by Dr Mary Harding, MRCGP
Frequently asked questions
What is the typical intelligence level of individuals with Turner Syndrome?
Most girls with Turner syndrome have normal intelligence. A few may experience learning difficulties, and in such cases, specialised assistance with schooling can be beneficial.
What is the life expectancy and quality of life for adults with Turner Syndrome?
For adults with Turner syndrome, life expectancy is only slightly reduced compared to the general population, and their overall quality of life is usually normal. With regular checks and appropriate treatment, especially for potential heart and blood vessel problems, individuals can lead happy and full lives.
How is osteoporosis managed in individuals with Turner Syndrome?
Osteoporosis, or 'thinning' of the bones, can occur later in life in individuals with Turner syndrome, often as a complication of a lack of oestrogen. This risk can be managed if oestrogen treatment is started early enough and taken continuously. Regular bone density scans are also advised to monitor bone health.
Are there specific dental issues associated with Turner Syndrome?
Due to the small size of the mouth in some girls with Turner syndrome, regular dental checks are recommended. These checks help manage problems with tooth abnormalities, particularly issues with dental occlusion, which refers to how the teeth meet when biting together.
Further reading and references
- Morgan T; Turner syndrome: diagnosis and management. Am Fam Physician. 2007 Aug 1;76(3):405-10.
- Baxter L, Bryant J, Cave CB, et al; Recombinant growth hormone for children and adolescents with Turner syndrome. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD003887.
- Gonzalez L, Witchel SF; The patient with Turner syndrome: puberty and medical management concerns. Fertil Steril. 2012 Oct;98(4):780-6. doi: 10.1016/j.fertnstert.2012.07.1104. Epub 2012 Aug 9.
- Lucaccioni L, Wong SC, Smyth A, et al; Turner syndrome - issues to consider for transition to adulthood. Br Med Bull. 2015 Mar;113(1):45-58. doi: 10.1093/bmb/ldu038. Epub 2014 Dec 22.
- Wong SC, Cheung M, Zacharin M; Aortic dilatation and dissection in Turner syndrome: what we know, what we are unclear about and what we should do in clinical practice. Int J Adolesc Med Health. 2014;26(4):469-88. doi: 10.1515/ijamh-2013-0336.
- Gawlik A, Malecka-Tendera E; Transitions in endocrinology: treatment of Turner's syndrome during transition. Eur J Endocrinol. 2013 Dec 27;170(2):R57-74. doi: 10.1530/EJE-13-0900. Print 2014 Feb.
- Turner Syndrome Support Society
- Shankar RK, Backeljauw PF; Current best practice in the management of Turner syndrome. Ther Adv Endocrinol Metab. 2018 Jan;9(1):33-40. doi: 10.1177/2042018817746291. Epub 2017 Dec 18.
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 21 Feb 2028
22 Feb 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in children's health
- Anxiety in children
- Baby-led weaning
- Breathing difficulties in children
- Dyslexia
- Erythema toxicum neonatorum
- Gastroenteritis in children
- Hydrocele in infants
- Nausea and vomiting
- Neonatal jaundice
- Perthes' disease
- Polio and polio vaccine
- Pyloric stenosis
- Right lower quadrant pain in children
- Rubella
- Squint in children
- Stammer
- Teething
- Treating newborn health problems
- Wilson's disease