Thyroid eye disease
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 14 Nov 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Overactive thyroid glandGoitreThyroid function testsThyroid scans and uptake testsAntithyroid medicines
Thyroid eye disease causes the muscles and soft tissues within the eye socket to swell. This pushes the eyeball forward and causes various eye symptoms, including bulging eyes. Treatment involves steps to protect the eye as the disease runs its course. This may involve use of eye drops to provide artificial lubricating tears, medicines and, in some cases, surgery. Thyroid eye disease is usually associated with an abnormality of thyroid gland function. This also needs to be treated.
At a glance
Thyroid eye disease is an autoimmune condition where eye socket tissues become inflamed and swollen.
This can cause bulging eyes, pain, redness, dryness, and double vision.
It is often linked to an overactive thyroid gland, particularly Graves' disease.
Not smoking can help reduce the severity of the condition.
Treatment aims to reduce inflammation, protect the eye surface, and may involve medicines or surgery.
Thyroid eye disease
In thyroid eye disease the muscles and fatty tissues within the eye socket (orbit) become inflamed and swollen, pushing the eyeball forward and affecting the movements of the eye.
This causes bulging eyes (what doctors call exophthalmos). In severe cases vision may be affected.
It is usually (but not always) associated with an overactive thyroid gland (hyperthyroidism) - and most often with one particular cause of an overactive thyroid gland, Graves' disease (Graves ophthalmology disease).
See the separate leaflet called Overactive thyroid gland (Hyperthyroidism).
Normal eye with muscles
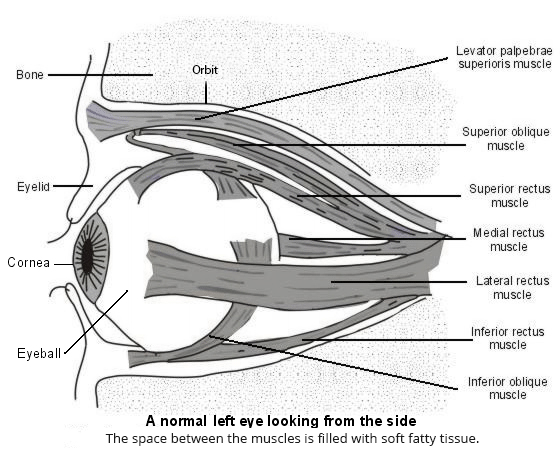
There is limited space inside the orbit so, as the tissues swell, the eyeball is pushed forwards. Usually this is mild, but in severe cases the eye is pushed far enough forward that the eyelids don't close as effectively. This leaves the clear window in the front part of the eye (the cornea) dry and unprotected. The eyeball also cannot move so easily, as the muscles that control it work less well. When the disease is very severe, the nerve connecting the eyeball to the brain can be compressed and damaged.
In thyroid eye disease there is an 'active phase' - a period of inflammation and swelling - followed by a healing response.
Thyroid eye disease is sometimes called other names such as thyroid ophthalmopathy, dysthyroid eye disease, Graves' ophthalmopathy or ophthalmic Graves' disease. However, a significant minority of cases are not associated with Graves' disease.
Thyroid eye disease symptoms
Symptoms are caused by the tissues of the eye socket swelling and pushing the eyeball forwards. The eye problems with thyroid eye disease include:
Aching (worse in the mornings) behind the eye, especially when looking up, down or sideways.
The front of your eyes can become red and irritated when the sensitive clear window of the eye (the cornea) is less well covered or lubricated by the eyelids.
You may have bulging eyes, giving you a staring or startled appearance (what doctors call exophthalmos).
You may have double vision (diplopia) as the muscles become too swollen to work properly.
In advanced disease, you may have blurred or double vision, and colours can appear less vivid.
Mild sensitivity to light (photophobia).
Swelling and redness of the eyelids.
Difficulty moving the eyes.
The two eyeballs are not always equally affected. You may have other non-eye symptoms due to the abnormal thyroid gland.
Thyroid eye disease

© Jonathan Trobe, M.D. - University of Michigan Kellogg Eye Center, CC BY 3.0, via Wikimedia Commons
Treatment of thyroid eye disease
Thyroid eye disease is a self-limiting disease: if left untreated, the inflammation will gradually go by itself. However, the physical changes caused by the swelling (such as eyeball bulge) may remain. This is because some of the tissues that have been stretched may not always return to their original form. The aim of treatment is mainly to limit inflammation and swelling occurring during the inflamed period and to protect the surface of the eye. There are also treatments for people whose tissues have not been able to return to their original form after the inflammation has settled.
Thyroid eye disease is managed by a specialist eye doctor (ophthalmologist) and the underlying thyroid problem by your own doctor or by a specialist in the hormone systems of the body (an endocrinologist).
Not smoking is very important, even if you already have thyroid eye disease, as this will reduce the severity.
Medicines
In the early phase of the disease and where the disease stays mild, artificial tears (ocular lubricants) may be enough.
If the disease progresses, you may need immunosuppressive medicines. These dampen down the immune system which is producing these abnormal antibodies.
Commonly used immunosuppressants are steroids such as prednisolone. You will be given some other medicines to counteract some of the side-effects of steroids, such as omeprazole, a medicine that protects the lining of the stomach.
If you have severe disease and the doctors are concerned about your sight, you may be admitted into hospital for a course of steroids administered through a drip.
Surgical treatment
About 5 in 100 people with thyroid eye disease have such severe disease that the optic nerve (connecting the back of the eyeball to the brain) is compressed. This can permanently damage your vision. If this is the case, the doctor may decide to organise decompression surgery. This is a procedure that creates a space within the eye socket (orbit) for the inflamed tissues to spread into. This relieves the pressure on the nerve.
Some people find that once the inflammation has settled, they are left with unacceptably bulgy eyes. In some cases surgery on the orbit will allow the eyeballs to settle back into the sockets.
Occasionally, surgery to the stretched muscles or to the lids is needed to help normal function.
Other types of treatment
If you develop double vision (diplopia), you may be referred to a specialist health professional who manages problems with eye muscles (an orthoptist). They may give you modified glasses that block off vision from one eye (like a patch) or put a special cover, called a prism, over one side to stop the diplopia.
Treatment using radiation (radiotherapy) may be used in some places on some people. The aim is to reduce the swelling in the eye. It is used alongside other forms of treatment.
A number of new treatments are being investigated.
Your doctors will also treat any abnormality of thyroid function with antithyroid medicines. This is usually with tablets but may also include radioactive iodine or, uncommonly, surgery to the thyroid gland. We know that good control of the thyroid function helps lessen the severity of thyroid eye disease. See the separate leaflet called Antithyroid medicines.
Understanding thyroid eye disease
The thyroid gland
The thyroid gland is a small butterfly-shaped gland sitting near the top of your windpipe (trachea) at the front of your neck. It has an important role in controlling the speed at which chemical reactions happen in the tissues throughout your body (metabolic rate). The thyroid gland can become overactive or underactive. This is most often due to an autoimmune disease.
Autoimmune thyroid disease
Thyroid eye disease is an autoimmune disease, most often occurring in association with an overactive thyroid gland (hyperthyroidism). The immune system normally makes small proteins (antibodies) to attack germs (for example, bacteria). In autoimmune disease, the immune system makes antibodies against tissues of the body. It is not clear why this happens. Some people have a particular tendency to develop autoimmune diseases.
Autoimmune thyroid disease occurs when the body's antibodies attack the thyroid gland. Graves' disease is an autoimmune thyroid disease which causes a swelling of the thyroid gland (called a goitre). See the separate leaflet called Goitre (Thyroid swelling). In some people, these same antibodies also attack the tissues around the eyeball, causing thyroid eye disease. It is not known why this happens in some people and not in others.
Who develops thyroid eye disease?
Thyroid eye disease is a rare condition. Each year it affects about 16 women and 3 men in every 100,000 people. Most of these people also have a problem with an overactive thyroid gland (hyperthyroidism) and have an underlying autoimmune condition. Occasionally, thyroid eye disease occurs when the thyroid gland appears to be working normally. However, people with an apparently normal thyroid gland at the time of thyroid eye disease have usually had abnormal thyroid function in the past or they go on to develop abnormal thyroid function in the future.
Thyroid eye disease generally occurs in middle age. Some people carry genes which make it more likely that they will develop thyroid eye disease. It is also more likely to develop if you smoke, particularly if you are a heavy smoker.
How is thyroid eye disease diagnosed?
Diagnosis can be made simply on examining your eyes if you already have a diagnosis of a thyroid gland problem.
Blood tests
Sometimes, blood tests are needed to back up the diagnosis. They look at how well the thyroid gland is functioning by measuring its chemical messengers (thyroid hormone levels) in your bloodstream. See the separate leaflet called Thyroid function tests. More specialised blood tests can be done to measure the antibodies in your blood.
Scans
Occasionally, thyroid scans and uptake tests need to be done to see how actively the thyroid gland is working. See the separate leaflet called Thyroid scans and uptake tests. If the doctors need to look at the amount of swelling in the eye socket (orbit), they may organise a magnetic resonance imaging (MRI) scan. This is used to show up which tissues have been most affected.
Other tests
Doctors will want to assess your general sight carefully. This will include how well you see colours and how good the vision out of the corner of your eye (your peripheral vision) is. They may also want to carry out an eye movement test to see how much the muscles have been affected. These assessments will be repeated throughout the course of the disease.
Frequently Asked Questions
Is there anything I can do?
Yes. Here are a few tips:
We know that one thing that makes this disease worse is smoking. If you smoke, see your GP about getting help to stop. Stopping smoking, even if you already have thyroid eye disease, will reduce the severity.
Sleeping propped up will help reduce the puffiness (congestion) around the eyes.
You may find bright light uncomfortable. Sunglasses will help.
If you are a driver and experience double vision, let the DVLA know. This is a legal requirement. Usually, they will contact your specialist eye doctor (ophthalmologist) for a report. If the double vision is well controlled with prisms, you may be declared fit to drive. Until then you should not drive.
Are there any complications from thyroid eye disease?
Most people do not develop permanent complications. However, where treatment is delayed or where the thyroid eye disease has been severe, there can be lasting effects. They are also more likely in older people, in those who smoke and in people with diabetes. Possible complications include:
Complications from the disease
Damage to the clear window of the eye (the cornea).
Permanent squint or double vision (diplopia).
Damage to the nerve of the eye, resulting in poor vision or colour appreciation.
Altered appearance (eyes more protruding).
Complications from treatment
Side-effects from the immunosuppressive medicines.
Side-effects from the surgery:
New double vision (about 15 in 100 people with thyroid eye disease).
Vision loss (fewer than 1 in 1,000 people with thyroid eye disease).
There are some other very rare complications that your surgeon will talk you through.
What is the outlook for thyroid eye disease?
Thyroid eye disease is a temporary but drawn-out illness which fades away by itself. The inflamed period tends to last months to years (usually about two years), after which there is a healing response. For most people the condition will be mild, needing lubricants and regular assessments only. For those with more severe disease, the outlook (prognosis) depends on how early it is diagnosed and how intensive the treatment is. About 1 in 4 people with severe disease will end up with reduced eyesight.
Dr Mary Lowth is an author or the original author of this leaflet.
Patient picks for Thyroid condtions

Hormones
Iodine deficiency
Iodine is essential for the body to make thyroid hormone. Low levels of iodine may cause an underactive thyroid gland and symptoms of hypothyroidism (eg, tiredness, constipation and weight gain). Iodine deficiency in pregnant women may cause problems for the baby, including learning disability. There has been a worldwide campaign to prevent iodine deficiency by using salt containing added iodine. However, iodine deficiency is still a widespread problem in many countries. Mild iodine deficiency may still affect some people in the UK.
by Dr Rosalyn Adleman, MRCGP

Hormones
Thyroid and parathyroid problems
This leaflet gives a brief overview of the thyroid and parathyroid glands and the common medical problems which can occur with these.
by Dr Caroline Wiggins, MRCGP
Frequently asked questions
Can thyroid eye disease lead to vision loss?
In severe cases, the optic nerve connecting the eyeball to the brain can be compressed and damaged, which can permanently impair vision. A small number of people, about 1 in 4 of those with severe thyroid eye disease, may experience reduced eyesight.
How long does the active phase of thyroid eye disease typically last?
Thyroid eye disease is a self-limiting condition with an 'active phase' of inflammation and swelling. This inflammatory period usually lasts for months to a couple of years, typically around two years, followed by a healing response.
Who is more likely to develop thyroid eye disease?
Thyroid eye disease commonly affects people in middle age, with genes playing a role in susceptibility. It is also more likely to develop in smokers, especially heavy smokers. Annually, it affects about 16 women and 3 men per 100,000, usually alongside an overactive thyroid gland due to an autoimmune condition.
What is the difference between thyroid eye disease and Graves' disease?
Thyroid eye disease is an autoimmune condition where the immune system attacks tissues around the eyeball. It is most often associated with an overactive thyroid gland (hyperthyroidism), and frequently, this hyperthyroidism is caused by Graves' disease. Graves' disease itself is an autoimmune thyroid condition where antibodies attack the thyroid gland, sometimes also affecting the eye tissues, leading to thyroid eye disease.
Can an individual have thyroid eye disease without an overactive thyroid gland?
While thyroid eye disease is usually, but not always, linked with an overactive thyroid gland, there are cases where it occurs when the thyroid gland appears to be functioning normally. However, individuals with a seemingly normal thyroid at the time of diagnosis have typically had abnormal thyroid function in the past or will develop it in the future.
Further reading and references
- Thyroid disease: assessment and management; NICE guidance (November 2019 - last updated October 2023)
- Rashad R, Pinto R, Li E, et al; Thyroid Eye Disease. Life (Basel). 2022 Dec 12;12(12):2084. doi: 10.3390/life12122084.
- Yoon JS, Kikkawa DO; Thyroid eye disease: From pathogenesis to targeted therapies. Taiwan J Ophthalmol. 2022 Jan 21;12(1):3-11. doi: 10.4103/tjo.tjo_51_21. eCollection 2022 Jan-Mar.
- Barbesino G, Salvi M, Freitag SK; Future Projections in Thyroid Eye Disease. J Clin Endocrinol Metab. 2022 Aug 8;107(Suppl_1):S47-S56. doi: 10.1210/clinem/dgac252.
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 13 Nov 2027
14 Nov 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in hormones
- 10-Week Menopause Course
- Acromegaly
- Acute pancreatitis
- Addison's disease
- Alternatives to HRT for menopause symptoms
- Chronic pancreatitis
- Diabetes insipidus
- Goitre
- Greene Menopause Scale
- Hormone replacement therapy (HRT)
- Hyperparathyroidism
- Hypoparathyroidism
- Iodine deficiency
- Ovarian cancer
- Overactive thyroid gland
- Pelvic pain in women
- Perimenopause
- Premature ovarian insufficiency
- Prolactinoma
- Vaginal dryness