Asthma
Peer reviewed by Dr Philippa Vincent, MRCGPLast updated by Dr Doug McKechnie, MRCGPLast updated 7 Feb 2025
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Asthma inhalersPeak flow meter for asthma
Asthma is a common condition that affects the airways. The typical symptoms are wheeze, cough, chest tightness, and shortness of breath. Symptoms can range from mild to severe. Treatment usually works well to ease and prevent symptoms.
Treatment is usually with inhalers. This leaflet gives a general overview of asthma. There are other separate leaflets in this series.
At a glance
Asthma is a condition that causes the airways in the lungs to narrow.
Common symptoms include coughing, wheezing, breathlessness, and chest tightness.
Symptoms are caused by inflammation in the airways, often triggered by various factors.
Inhalers are the main treatment and help prevent symptoms for most people.
Seek medical help if you suspect you or your child has asthma or if existing symptoms worsen.
A severe asthma attack needs emergency medical treatment; call for an ambulance immediately.
An annual review with a doctor or nurse and a written action plan can help manage asthma.
In this article:
Video picks for Asthma
Continue reading below
What is asthma?
Asthma is a condition that affects the smaller airways (bronchioles) of the lungs. From time to time the airways narrow (constrict) in people who have asthma.
This causes the typical symptoms of asthma (see below). The extent of the narrowing, and how long each episode lasts, can vary greatly.
About 8 million people in the UK have asthma, which is about 12 in every 100 people. Asthma can start at any age but it most often starts in childhood.
Asthma runs in some families but many people with asthma have no other family members affected.
Asthma symptoms
Back to contentsCommon asthma symptoms are:
Coughing. This is usually a dry cough, and often made worse by asthma triggers like cold air, exercise, or allergens.
Wheezing. A wheeze is a high-pitched whistling sound made when you breathe, caused by air flowing through narrowed airways in the lungs.
Breathlessness. This means that you feel out of breath, are finding it difficult to get enough air, or are breathing harder and faster than normal.
Feeling of chest tightness. Some people feel like their chest feels tight, or like there is a dull ache or sharp pain in the chest.
Asthma symptoms can range from mild to severe between different people and at different times in the same person. Each episode of asthma symptoms could last for an hour or so, or persist for days or weeks unless treated.
Mild untreated asthma
Mild asthma symptoms can occur from time to time. For example, a mild wheeze and a cough with a cold or a chest infection. Mild symptoms may also occur during the hay fever season, or with exercise.
Most of the time there may be no asthma symptoms at all. A child with mild asthma may have an irritating cough each night but is often fine during the day.
Moderate untreated asthma
Typically there are episodes of wheezing and coughing from time to time. Sometimes breathless may occur. There is usually spells without symptoms. However, wheezing tends to occur for some of the time on most days.
Symptoms are often worse at night, or first thing in the morning. Symptoms may include waking some nights coughing or with a tight chest.
Young children may not have typical symptoms. It may be difficult to tell the difference between asthma and recurring chest infections in young children.
Severe asthma attack
A severe asthma attack causes severe wheezing, a tight chest and difficulty in breathing. It may be difficult to talk because of being severely breathless.
People with a severe asthma attack usually look, and feel, very unwell. A severe asthma attack needs emergency medical treatment.
Severe symptoms may develop suddenly in some people who usually just have mild or moderate symptoms.
When to see a doctor about asthma
It is very important to see a doctor if there is any concern that an adult or child has asthma. Several conditions can cause similar symptoms, so it's important to get a proper diagnosis and correct treatment. The doctor will usually be able to diagnose asthma by asking about symptoms and carrying out some simple tests.
If you already have asthma, see a doctor or nurse if the symptoms become worse and cannot be controlled by the usual treatments.
People with asthma should also have a review each year at their GP surgery to check up on the asthma, and how it is affecting them.
A severe asthma attack, especially with difficulty breathing that does not respond to usual asthma treatment, is a medical emergency. Call an ambulance immediately.
Continue reading below
What causes asthma?
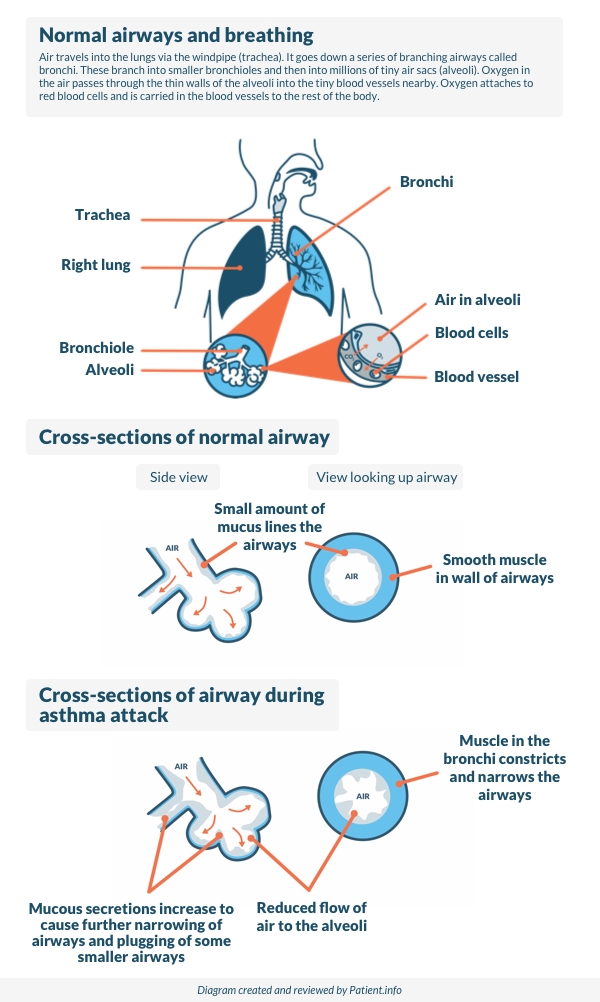
Back to contentsThe symptoms of asthma are caused by inflammation (swelling) in the airways of the lungs, which may be triggered by different things in different people. The inflammation causes the muscles around the airways to squeeze (contract).
This causes narrowing of the airways. It is then more difficult for air to get in and out of the lungs. This leads to wheezing and breathlessness. The inflammation also causes the lining of the airways to make extra mucus which causes cough and further blockage to the airflow.
The following diagram below shows how an episode of asthma develops.
How asthma develops
Asthma symptoms may flare up from time to time. There is often no obvious reason why asthma symptoms flare up.
Asthma triggers
However, some people find that symptoms are triggered, or made worse, in certain situations. It may be possible to avoid certain triggers, which may help to reduce symptoms. Things that may trigger asthma symptoms include the following:
Infections - particularly colds, coughs and chest infections.
Pollens and moulds - asthma is often worse in the hay fever season.
Exercise - getting asthma symptoms with exercise often means asthma is undertreated. If it happens, it may be necessary to step up usual preventer treatment (see below). Use an inhaler before exercise to prevent symptoms from developing.
Certain medicines - for example, about 1 in 50 people with asthma are allergic to aspirin, which can trigger symptoms. Other medicines that may cause asthma symptoms include:
Anti-inflammatory painkillers such as ibuprofen (for example, Nurofen®), diclofenac, etc.
Beta-blockers such as propranolol, atenolol, or timolol. This includes beta-blocker eye drops used to treat glaucoma.
Smoking and cigarette fumes - smoking makes asthma much worse and every effort should be made to stop smoking. Passive smoking can make asthma worse too. Even where adults smoke away from children, smoke on clothes, hair, etc, may make asthma worse.
Other fumes and chemicals - for example, fumes from paints, solvents and pollution. The increase in air pollution may be a reason why asthma is becoming more common. Details about current levels of air pollution, are available from The Daily Air Quality Index, which can be found on the Department for Environment Food and Rural Affairs (DEFRA) website (see further reading for link).
Certain pillows and mattresses - feathers in pillows may trigger symptoms. It is thought that some people develop asthma symptoms from chemicals (isocyanates/methyl ethyl ketones, etc) that are emitted in very low quantities from memory foam pillows and mattress toppers.
Emotion - asthma is not due to 'nerves'; however, such things as stress, emotional upset, or laughing may trigger symptoms.
Allergies to animals - for example, pet cats and dogs, and horses. Some people notice that their symptoms become worse when close to certain animals.
House dust mites - this is a tiny creature which lives in mattresses and other fabrics around the home. Allergy to house dust mites may make symptoms worse. It is impossible to get rid of house dust mite completely.. However, if symptoms are difficult to control with treatment and allergy to house dust mite has been confirmed, it may be worth considering trying to reduce their number. See the separate leaflet called House dust mite and pet allergy for more details.
Some foods - this is uncommon. Food is not thought to be a trigger in most cases.
Some people only develop asthma symptoms when exposed to a certain trigger - for example, exercise-induced asthma. However, there are some people who only develop symptoms when they exercise; the rest of the time they are fine. Another example is that some people only develop symptoms when exposed to specific chemicals.
Asthma treatment
Back to contentsFor most people with asthma, the symptoms can be prevented most of the time with treatment. This allows a person with asthma to get on with a normal life at school, work, sport, etc.
Inhalers. Inhalers are the main treatment for people with asthma. Inhalers deliver a small dose of medicine directly to the airways. The dose is enough to treat the airways. However, the amount of medicine that gets into the rest of the body is small so side-effects are unlikely, or minor.
There are various inhaler devices made by different companies. Different ones suit different people. A doctor or nurse will advise on the different types. See the separate leaflet called Asthma inhalers for more details.
Bone strength (density) may be reduced following long-term use of high doses of inhaled steroids. Therefore people who regularly use steroid inhalers for asthma need to make sure they have a good supply of calcium in their diet. Milk and dairy are good sources of calcium. Other good dietary sources of calcium include bread, some vegetables (curly kale, okra, spinach and watercress) and some fruits (for example, dried apricots). See the separate leaflet called Preventing steroid-induced osteoporosis for more details.
Inhalers contain different types of medication. Inhalers can have one medication or a combination of different ones. There are three main types of medication in inhalers: short-acting relievers, inhaled steroids or preventers, and long-acting relievers or bronchodilators:
Short-acting relievers. These contain a medicine called a short-acting bronchodilator. These medications relax the muscles in the airways, causing the airways to open up quickly. The effect lasts for a short time - usually only a few hours. There are several different reliever medicines - for example, salbutamol (Ventolin®)and terbutaline.
Short-acting relievers only treat the symptoms of asthma and not the underlying cause, which is inflammation (swelling) in the airways. People with asthma shouldn't use short-acting relievers as their only asthma treatment. It is much better to use an anti-inflammatory reliever, or to use a regular preventer (inhaled steroid) alongside a short-acting reliever (see below).
If you have asthma and only use a short-acting reliever inhaler, speak to your doctor or nurse about a change in treatment.
Inhaled steroids in preventer inhalers. This is taken every day to prevent symptoms from developing. The medicine commonly used in preventer inhalers is a steroid. Steroids work by reducing the inflammation in the airways. When the inflammation has gone, the airways are much less likely to become narrow and cause symptoms. It takes 7-14 days for the steroid in a preventer inhaler to build up its effect. Therefore, it will not give any immediate relief of symptoms. However, after a week or so of treatment, the symptoms have often gone, or are much reduced. It can take up to six weeks for maximum benefit. The preventer inhaler should be used every day even when symptoms have gone - this is to prevent symptoms from coming back. A reliever inhaler should then not be needed very often (if at all).
Long-acting bronchodilators. These are sometimes added alongside inhaled steroids in preventer inhalers. Long-acting bronchodilators relieve symptoms as they widen the lung airways but work for longer than reliever inhalers. The medicines in these inhalers work for up to 12 hours after each dose has been taken. They include salmeterol and formoterol. (Some brands of inhaler contain a steroid plus a long-acting bronchodilator for convenience.) A long-acting bronchodilator may be needed if symptoms are not fully controlled by the preventer inhaler alone.
Spacer devices. These devices are used with some types of inhaler. They are commonly used by children; however, many adults also use them. A spacer is like a small plastic chamber that attaches to the inhaler. It holds the medicine like a reservoir when the inhaler is pressed. A valve at the mouth end makes sure that the medicine is kept within the spacer until breathing it in. When breathing out, the valve closes. Spacers make it much easier to use inhalers so that the medication gets into the lungs, where it needs to be. A face mask can be fitted on to some types of spacers instead of a mouthpiece. This is sometimes done for babies and young children who can then use the inhaler simply by breathing in and out normally through the mask.
Tablets to open up the airways. Most people do not need tablets, as inhalers usually work well. However, in some cases a tablet (or medicine in liquid form for children) is prescribed in addition to inhalers if symptoms are not fully eased by inhalers alone. Various tablets may be used which aim to open up the airways. Some young children use liquid medication instead of inhalers. Tablets used for asthma include:
Leukotriene receptor antagonists (LTRAs). Chemicals called leukotrienes are produced in some people who have asthma which is triggered by an allergic reaction (for example, pollen) or sometimes exercise. LTRAs such as montelukast act by blocking the action of these chemicals. Montelukast comes in the form of tablets or granules. In people whose asthma is not well controlled by a reliever inhaler and a preventer inhaler, NICE recommends trying an LTRA before adding a long-acting bronchodilator inhaler.
Steroid tablets. A short course of steroid tablets (such as prednisolone) is sometimes needed to ease a severe or prolonged attack of asthma. Steroid tablets are good at reducing the inflammation in the airways. For example, a severe attack may occur with a cold or a chest infection. Some people worry about taking steroid tablets. However, a short course of steroid tablets (for a week) usually works very well and is unlikely to cause side-effects. Most of the side-effects caused by steroid tablets occur if they are taken for a long time (more than several months), or after a lot of short courses of high-dose steroids over a short period of time.
Biologic therapies. Monoclonal antibodies are biologic treatments used for treating many diseases. They work by targeting specific cells and proteins to make the disease better. In asthma, they work by interfering with the immune system to reduce inflammation in the airways. These are medicines that are only used in a small number of people who have severe persistent allergic asthma that have not been controlled by other treatments. So, it is not a common treatment.
Biologic therapies
Currently there are six treatments used in the NHS and recommended by NICE:
Mepolizumab (Nucala).
Reslizumab (Cinqaero®).
Benralizumab (Fasenra®).
Omalizumab (Xolair®).
Dupilumab (Dupixent®).
Tezepelumab (Tezspire®).
They are most commonly given by injection. These treatments can only be started by a specialist. Each medication has its own rules on when they can be started by a specialist. If needed, an asthma specialist will go into much more detail about that specific one.
What are the dosages of treatment?
Everyone is different. The correct dose of a preventer inhaler is the lowest dose that prevents symptoms. A doctor may prescribe a high dose of a preventer inhaler at first, to 'get on top of symptoms' quickly. When symptoms have gone, the dose may then be reduced by a little every few weeks. The aim is to find the lowest regular dose that keeps symptoms away.
Some people with asthma put up with symptoms. They may think that it is normal still to have some symptoms even when they are on treatment. A common example is a night-time cough which can cause disturbed sleep.
But, if this occurs and symptoms are not fully controlled, it is very important to see a doctor or nurse for an asthma review. Symptoms can often be prevented - for example, by adjusting the dose of the preventer inhaler, or by adding in a long-acting bronchodilator.
A typical treatment plan for asthma
The recommendations on asthma treatment plans have recently changed. A common treatment plan for someone with asthma, especially children, is:
A preventer inhaler (usually a steroid inhaler), taken each morning and at bedtime. This usually prevents symptoms throughout the day and night.
A reliever inhaler may be needed now and then if breakthrough symptoms occur. For example, if symptoms flare up with a cough or cold.
There is a newer way of using inhalers, though, which seems to work better for many people, called maintenance-and-reliever therapy, or MART. MART involves:
Using a single inhaler that contains a bronchodilator or reliever called formeterol, and an inhaled steroid. Formeterol is a long-acting reliever but starts to work quickly, meaning it gives quick relief from symptoms.
The inhaler should be used regularly (usually twice a day), and also used if asthma symptoms get worse or if someone is having an asthma attack.
Many people are switching over to MART instead of using two separate reliever and preventer inhalers, as it is simpler and seems to work better for treating asthma and preventing asthma attacks.. Speak to your doctor or nurse if you would like to see if it's an option for you.
People with asthma should have a written asthma action plan agreed with their doctor or nurse, which explains how to use their inhalers, and what to do if their symptoms get worse.
Continue reading below
Asthma action plan
Back to contentsAn asthma action plan is a plan agreed by anyone with asthma with a doctor or nurse. The plan enables changes to the dose of the inhalers, depending on symptoms and/or peak flow readings. The plan is tailored to each individual. It is written down, usually on a standard form, so that it's clear what to do at any time.
The plan should include:
What to do when unwell - for example, with a cold - and when to seek help.
What to do if symptoms become worse with hay fever or exercise.
A discussion on ways to reduce exposure to air pollution, both indoors and outdoors. If asthma is triggered by household sprays, air fresheners or aerosols, it is important to avoid using them or use non-spray alternatives instead. Mould and house dust mites in the home can also make asthma worse. If problems with mould in the home, a doctor can sometimes help request a housing assessment from the local authority.
Research studies suggest that people who complete personal asthma action plans find it easier to manage their asthma symptoms and that their plan helps them to go about their lives as normal. Asthma+Lung UK provides asthma action plans which can be downloaded (see 'Further Reading' below).
Asthma diagnosis
Back to contentsIn the past, many cases of asthma were diagnosed on the basis of typical symptoms and without any tests. However, this can lead to mistakes, so it's now recommended that people should also have one or more tests to confirm asthma before making the diagnosis.
It's not always possible to do these tests straight away, so doctors might recommend trying asthma treatment anyway whilst waiting for tests, particularly if someone has troublesome symptoms or is very unwell.
There are various different tests that might be used, such as:
FeNO test. FeNO stands for fractional exhaled nitrous oxide. It measures the amount of nitrous oxide in the breath. Raised levels of nitrous oxide mean that there is inflammation in the airways of the lungs, which can be used to confirm a diagnosis of asthma. It is sometimes also used as a monitoring test for people with asthma; if it is raised, it suggests that they are not getting enough inhaled steroid to reduce inflammation in the lungs. Some GP surgeries have access to a FeNO test, but others may need to refer to a specialist to get it.
A blood test for eosinophils. Eosinophils are a type of white blood cell that can be raised due to several different conditions, including asthma. If someone has typical symptoms of asthma, and a raised blood eosinophil level, this confirms the diagnosis of asthma.
Spirometry. Spirometry is a test which measures how much air can be blown out into a machine called a spirometer. Two results are important:
The amount of air that can be blown out in one second - called forced expiratory volume in one second (FEV1).
The total amount that can be blown out in one breath - called forced vital capacity (FVC).
Age, height and sex affect lung volume. So, spirometry results are compared with a graph showing the average predicted for age, height and sex. A value is calculated from the amount of air that can be blown out in one second divided by the total amount of air that can be blown out in one breath (called FEV1:FVC ratio). A low value indicates narrowed airways which are typical in asthma (but a low value can occur in other conditions too). Therefore, spirometry may be repeated after treatment with a reliever inhaler. An improvement in the value after treatment to open up the airways, is typical of asthma. Note: spirometry may be normal in people with asthma who do not have any symptoms when the test is done. Remember, the symptoms of asthma typically come and go. Therefore, a normal result does not rule out asthma. However, if symptoms suggest asthma, ideally the test should be repeated when symptoms are present.
See the separate leaflet called Spirometry for more details.
Assessment with a peak flow meter. This is an alternative test. A peak flow meter is a small device to blow into. A doctor or nurse will demonstrate how to use a peak flow meter. It measures the speed of air that can be blow out of the lungs. If the airways are narrowed, the peak flow reading will be lower than expected for age, height and sex. Untreated asthma will usually cause low and variable peak flow readings. Also with asthma, peak flow readings in the morning are usually lower than in the evening. It is useful to keep a diary of peak flow readings over about two weeks. Typically, a person with asthma will usually have low and variable peak flow readings over several days. Peak flow readings improve when the narrowed airways are opened up with treatment. Regular peak flow readings can be used to help assess how well the treatment is working. See the separate leaflet called Peak Flow Meter for Asthma and our editorial article called Peak flow diary for more details.
Other tests. If the diagnosis remains in doubt then a specialist may perform further, more complex tests. However, these are not needed in most cases. Although not recommended for diagnosis, allergy tests may be used to identify any asthma triggers after a diagnosis of asthma has been made. See also the separate leaflet called Allergies.
Diagnosing asthma in children under 5 years old. Children under 5 often can't do the tests above accurately. So guidelines recommend that if a doctor suspects that an under 5-year-old has asthma, they offer treatment based on symptoms. However, once they reach the age of 5, they should have one or more of the tests above if they still have symptoms.
The tests above can sometimes be normal even in people who do have asthma. The results can also be affected by asthma treatment - they may be normal if the treatment is working well. So a normal result doesn't necessarily mean that someone does not have asthma; the results need to be interpreted looking at the overall picture of your symptoms and response to treatment.
Common Questions
Back to contentsDoes asthma go away?
For many people, asthma is a life-long condition. There is no cure for asthma, but daily treatment can keep asthma under good control.
Asthma does sometimes go away in some people. About half of children with asthma find that asthma symptoms go away completely by the time they are adults. However, for some of them, asthma symptoms return later in life, particularly if they are exposed to an asthma trigger such as pollution or smoking.
Some adults also find that their asthma improves with time; studies suggest that, in around 1 in 10 to 3 in 10 adults with asthma, their asthma symptoms improve and may disappear over decades. This is more likely in people with mild asthma, and in people who started treatment early on for their asthma.
For many adults, asthma is variable with some good spells and some spells that are not so good. Some people are worse in the winter months and some are worse in the hay fever season. Although not curable, asthma is treatable. Stepping up the treatment for a while during bad spells will often control symptoms.
Don't underestimate asthma
Because modern management is so effective, many people with asthma are well controlled. However, this has led to the belief that asthma is a mild and even trivial condition.
The fact is that when asthma goes wrong, it can do so quickly. Deaths from asthma are rising. More than 1,400 people died from asthma in 2020, representing an increase of nearly 4% over the previous year..
There are several things to lower the risk of asthma getting out of control:
Make sure you are accessing basic asthma care. This should involve at least an annual review from your GP or asthma nurse, including an inhaler technique check. You should be given a written asthma action plan.
Take your medication as prescribed.
If you develop symptoms which are not responding to your action plan, seek advice from a healthcare professional immediately.
"It's only asthma" is not a phrase that should pass anybody's lips.
Is asthma genetic?
Asthma is a complex condition with lots of different causes. Genetics aren't the only cause, but they might play a role. People with a family history of asthma are more likely to get asthma themselves. It's likely that people inherit a number of different gene variants which make them more likely to get asthma - for example, they might be more vulnerable to environmental triggers for asthma.
Is asthma a disability?
Asthma can be a disability, depending on how it is affecting someone.
In the UK, a disability is defined by the Equality Act 2010 as a condition that has a substantial and long-term adverse effect on a person's ability to carry out normal day-to-day activities.
So, someone with well-controlled asthma who has little or no symptoms is unlikely to be considered as having a disability, but someone whose asthma is significantly affecting their day-to-day life might be.
Silent asthma attack symptoms
A 'silent' asthma attack is when someone has an asthma attack but without the typical symptom of feeling or sounding wheezy. They might not realise that they are having an asthma attack, and this can delay them getting treatment.
Symptoms of a silent asthma attack can include:
Feeling breathless, short of breath, or having difficulty breathing.
Feeling tightness in the chest.
Coughing.
Feeling very fatigued (tired) or exhausted.
Breathing harder or faster than normal.
Some people with asthma find it really hard to tell that they are having an asthma attack until they become extremely unwell. This can happen in brittle asthma.
Can you develop asthma as an adult?
Asthma can develop at any age, although it's more common to develop in childhood. Asthma that develops in adulthood is called adult-onset asthma.
Some other general points about asthma
It is vital to learn how to use inhalers correctly. In some people, symptoms persist simply because they do not use their inhaler properly and the medicine from the inhaler does not get into the airways properly. See a pharmacist or practice nurse if you are not sure if you are using asthma inhalers properly.
See a doctor or nurse if symptoms are not fully controlled, or if they are getting worse. For example, if:
A night-time cough or wheeze is troublesome.
Sport is being affected by symptoms.
Peak flow readings are lower than normal.
A reliever inhaler is needed more often than usual.
An adjustment in inhaler timings or doses may control these symptoms.See a doctor urgently if you develop severe symptoms that are not eased by a reliever inhaler. In particular, if having difficulty talking due to shortness of breath. This may need emergency treatment with high-dose reliever medicine and other treatments, sometimes in hospital. A severe asthma attack can be life-threatening. In this case, call for an ambulance.
Patient picks for Asthma

Chest and lungs
Asthma Control Test (ACT)
Asthma is a long-term condition that affects around 5.4 million people in the UK. While medicines and inhalers are effective at controlling symptoms, many people are unsure whether their asthma is truly under control. The Asthma Control Test (ACT) is a quick, evidence-based way to check how well your asthma is managed in daily life.
by Patient infomatics team

Chest and lungs
Asthma inhalers
An inhaler is a device containing a medicine that is taken by breathing it in (inhaling). Inhalers are the main treatment for asthma and help to control asthma symptoms. There are many different types of inhaler. This leaflet gives information on the medicines inside inhalers, the types of inhaler device and some general information about inhalers. This leaflet is only about inhalers for asthma. It is important to recognise that the same inhalers can be used in other medical conditions (for example, chronic obstructive pulmonary disease) but that the way they are used may be different.
by Dr Doug McKechnie, MRCGP
Frequently asked questions
What is the difference between mild, moderate, and severe asthma symptoms?
Asthma symptoms can vary in intensity. Mild symptoms might include an occasional cough or mild wheeze, possibly with a cold or during hay fever season, and are often absent most of the time. Moderate symptoms involve more frequent episodes of wheezing and coughing, sometimes with breathlessness, often worse at night or in the morning. A severe asthma attack, however, presents with significant wheezing, chest tightness, and difficulty breathing, making it hard to talk, and requires immediate emergency medical attention.
How do doctors diagnose asthma in young children, especially if they can't do the standard tests?
Diagnosing asthma in children under 5 is challenging because they often cannot perform the required breathing tests accurately. In these cases, doctors rely more on the child's symptoms. If asthma is suspected, treatment based on their symptoms might be started. Once a child reaches age 5, if symptoms persist, they should then have one or more of the standard diagnostic tests like FeNO, blood tests for eosinophils, or spirometry.
Are there specific foods that can trigger asthma symptoms?
While uncommon, some people can find that certain foods trigger their asthma symptoms. However, food is generally not considered a trigger in most asthma cases.
What should I do if my regular asthma treatment isn't controlling my symptoms effectively?
If your asthma symptoms are not fully controlled, or if they worsen despite your usual treatment, it's very important to see a doctor or nurse for an asthma review. This is especially true if you have a troubling night-time cough or wheeze, if sports are affected by symptoms, if your peak flow readings are lower than normal, or if you need your reliever inhaler more often than usual. It may be possible to adjust your inhaler timings or doses, or a different treatment like a long-acting bronchodilator might be added, to get your symptoms under control.
What is a spacer device and why is it used with inhalers?
A spacer device is a small plastic chamber that attaches to an inhaler. It acts as a reservoir for the medicine when the inhaler is pressed, and a valve ensures the medicine stays within the spacer until breathed in. Spacers improve the delivery of medication to the lungs, making inhalers easier to use, especially for children, but many adults also use them. Some spacers can also have a face mask attached for babies and young children to breathe in normally.
Can emotions like stress or laughing bring on asthma symptoms?
While asthma is not caused by 'nerves', certain emotions, such as stress, emotional upset, or even laughing, can sometimes trigger asthma symptoms or make them worse.
Is it true that I should get a flu jab if I have asthma?
Yes, if you have asthma, it is important to have an influenza immunisation (flu jab) every autumn. This helps protect you from the flu, which can potentially worsen asthma symptoms.
Further reading and references
- Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN); NICE guideline (November 2024)
- Global Initiative for Asthma (GINA)
- Asthma + Lung UK
- British guideline on the management of asthma; Scottish Intercollegiate Guidelines Network (SIGN), British Thoracic Society (BTS), NHS Scotland (2003 - revised July 2019)
- Corticosteroids - inhaled; NICE CKS, May 2020 (UK access only)
- Air pollution forecast; Department for Environment Food and Rural Affairs (DEFRA)
- Indoor air quality at home. NICE guideline [NG149], January 2020
- Asthma; NICE Clinical Knowledge Summary. January 2025 (UK access only)
- Your asthma action plan; Asthma and Lung UK.
Continue reading below
About the authorView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
About the reviewerView full bio

Dr Philippa Vincent, MRCGP
General Practitioner, Medical Author
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent is an NHS GP working in North London.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 6 Feb 2028
7 Feb 2025 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.