Acute abdomen
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Colin Tidy, MRCGPLast updated 18 Jun 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find the Abdominal pain article more useful, or one of our other health articles.
Synonym: acute abdominal pain
See also the separate Abdominal pain article.
What is acute abdomen?
The term 'acute abdomen' represents a rapid onset of severe symptoms that may indicate life-threatening intra-abdominal pathology.
Pain is usually a feature but is not always the case. A pain-free acute abdomen is more likely in children and the elderly.
The differential diagnosis is extremely wide and definitive diagnosis is often difficult, particularly in primary care. This is due to the many different organs within the peritoneal cavity and the potential for referred pain.
Abdominal pain is a common problem, ranking in the top three symptoms of patients presenting to accident and emergency departments, but only a few of those patients will have an acute abdomen.
Management of the acute abdomen in primary care should focus on careful assessment to reach a differential diagnosis list, with close attention paid to symptoms and signs that may indicate a need to investigate the situation further in hospital.
The clinical scenario can change rapidly and conclusions previously reached by you or your colleagues may need to be revised as events evolve.
This article will concentrate on diagnosing the important causes of the acute abdomen in primary care/emergency department settings.
Causes of acute abdomen
This list is far from exhaustive but is a useful aide-mémoire for those conditions commonly seen in the community:12
Intestinal obstruction, including paralytic ileus (adynamic obstruction).
Gastrointestinal (GI) haemorrhage.
Non-surgical disease - eg, myocardial infarction, pericarditis, pneumonia, sickle cell crisis, hepatitis, inflammatory bowel disease, opiate withdrawal, typhoid, acute intermittent porphyria, HIV-associated lymphadenopathy or enteritis.
Classification of causes according to site of pain
Another way to consider the causes of an acute abdomen is by classifying them according to the area of the abdomen most affected by pain (again, the list is not exhaustive):
Acute abdomen
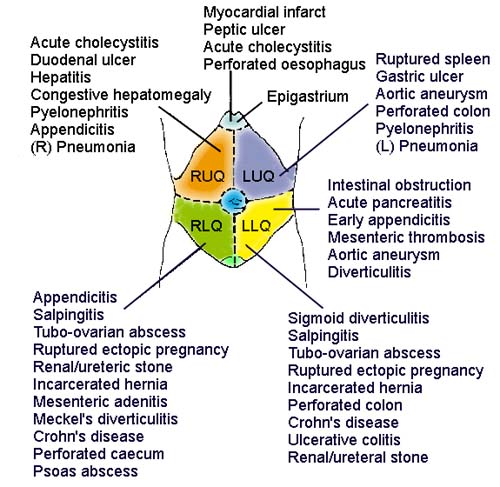
See the separate articles covering Epigastric pain, Left iliac fossa pain, Right iliac fossa pain, Left upper quadrant pain, Right upper quadrant pain, Pelvic pain and Loin pain.
Assessment
Initial impression/observation
Assess and manage Airway, Breathing and Circulation (ABC) as the priority.
Note whether the patient looks ill, septic or shocked.
Note whether they are lying still (think peritonitis) or rolling around in agony (think intestinal, biliary or renal colic)?
In an emergency department setting: if there are signs that the patient is shocked or acutely unwell, assess quickly but carefully and arrange any early investigations.
In a community setting: make arrangements for rapid transfer to hospital for further assessment.
History
This should cover the following points:
Demographic details, occupation, recent travel, history of recent abdominal trauma.
Pain:
Onset (including whether new pain or previously experienced).
Site (ask the patient to point), localised or diffuse.
Nature (constant/intermittent/colicky).
Radiation.
Severity.
Relieving/aggravating factors (eg, if worsened by movement/coughing, suspect active peritonitis; pancreatitis is relieved by sitting forward).
Associated symptoms:
Vomiting and the nature of vomitus (undigested food or bile suggests upper GI pathology or obstruction; faeculent vomiting suggests lower GI obstruction).
Haematemesis or melaena.
Stool/urine colour.
New lumps in the abdominal region/groins.
Eating and drinking - including when the patient's last meal occurred.
Bowels - including presence of diarrhoea, constipation and ability to pass flatus.
Fainting, dizziness or palpitations.
Fever/rigors.
Rash or itching.
Urinary symptoms.
Recent weight loss.
Past medical and surgical history/medication.
Gynaecological and obstetric history:
Contraception (including intrauterine contraceptive device (IUCD) use).
Last menstrual period.
History of sexually transmitted infections/pelvic inflammatory disease.
Previous gynaecological or tubal surgery.
Previous ectopic pregnancy.
Vaginal bleeding.
Drug history and allergies - including any complementary medication.
Examination
See also the separate Abdominal examination article.
Pulse, temperature and blood pressure.
Assess respiratory rate and pattern. Patients with peritonitis may take shallow, rapid breaths to reduce pain.
If there is altered consciousness, check Glasgow Coma Scale (GCS) or AVPU (Alert, Voice response, Pain response, Unconscious) scale.
Inspection:
Look for evidence of anaemia/jaundice.
Look for visible peristalsis or abdominal distension.
Look for signs of bruising around the umbilicus (Cullen's sign - this can be present in haemorrhagic pancreatitis and ectopic pregnancy) or flanks (Grey Turner's sign - this can be present in retroperitoneal haematoma).
Assess whether the patient is dehydrated (skin turgor/dry mucous membranes).
Auscultation:
Auscultate the abdomen in all four quadrants.
Absent bowel sounds suggest paralytic ileus, generalised peritonitis or intestinal obstruction. High-pitched and tinkling bowel sounds suggest subacute intestinal obstruction.
Intestinal obstruction can also present with normal bowel sounds.
If there is reason to suspect aortic aneurysm, listen carefully for abdominal and iliac bruits.
Percussion:
Percuss the abdomen to assess whether swelling/distension might be due to bowel gas or ascites.
Patients who display tenderness to percussion are likely to have generalised peritonitis and this should act as a red flag for serious pathology.
Assess for shifting dullness and fluid thrill.
Percussion can also be used to determine the size of an abdominal mass/extent of organomegaly.
Palpation:
Palpate the abdomen gently, then more deeply, starting away from the pain and moving towards it.
Feel for masses, tenderness, involuntary guarding and organomegaly (including the bladder).
Test for rebound tenderness.
Examine the groins for evidence of herniae.
Always examine the scrotum in men, as pain may be referred from unrecognised testicular pathology.
Check supraclavicular and groin lymph nodes.
Further examination:
Perform rectal or pelvic examination as needed, with an appropriate chaperone in attendance.
Check lower limb pulses if there could be an abdominal aortic aneurysm.
Dipstick urine and send for culture if appropriate.
In a woman of childbearing age, assume that she is pregnant until proven otherwise - perform a pregnancy test.
Examine any other system that might be relevant - eg, respiratory, cardiovascular.
Prehospital/emergency department care of suspected acute abdomen
Keep the patient nil by mouth.
Apply oxygen as appropriate.
Intravenous (IV) fluids: set up immediately if the patient is shocked and the equipment is available. Send blood for group and save/crossmatch and other blood tests as appropriate.
Consider passing a nasogastric (NG) tube if severe vomiting occurs, there are signs of intestinal obstruction or the patient is extremely unwell and there is danger of aspiration.
Analgesia: the previous practice was to withhold analgesia until surgical review, but a surgical abdomen is very painful and is likely only to be adequately relieved by parenteral opiates - eg, morphine. One recent review showed that opiate administration may alter physical examination findings, but these changes result in no significant increase in management errors.3. Another study showed that morphine safely provides analgesia without impairing diagnostic accuracy.4 A Cochrane review also supported the use of analgesia before assessment by a surgeon.5
Antiemetic: avoid using this as a symptomatic treatment without considering a diagnosis in a community setting.
Antibiotics: if systemic sepsis, or peritonitis, or severe urinary tract infection (UTI) is suspected. IV cephalosporin plus metronidazole are commonly used in acutely unwell patients in whom peritonitis is suspected.
Arrange urgent surgical/gynaecological review as appropriate.
Arrange investigations such as ECG if a medical cause is likely.
Admit: if surgery is considered likely, if the patient is unable to tolerate oral fluids, for pain control, if a medical cause is possible or if IV antibiotics are required.
Diagnosing acute abdomen (investigation)
This is mainly relevant to patients being assessed in emergency departments or secondary care.
With the exception of a urinary pregnancy test and urine dipstick, there are few tests that are useful in the community assessment of the patient with acute abdominal pain.
On the whole, if you are concerned enough to be ordering blood tests or imaging, the patient should be referred to secondary care.
The following tests are often used but can be nonspecific and must be interpreted in the clinical context and with appropriate medical/surgical expertise:
Blood tests: FBC, U&Es, LFTs, amylase, glucose, clotting, and occasionally calcium; arterial blood gas (pancreatitis).
'Group and save' or crossmatch.
Blood cultures.
Pregnancy test in women of childbearing age.
Urinalysis.
Radiology - abdominal X-ray (supine), CXR (erect, looking for gas under the diaphragm), intravenous pyelogram (IVP), CT scan, ultrasound scan, as appropriate.
Consider ECG and cardiac enzymes.
Peritoneal lavage if there is a history of abdominal trauma.
Laparoscopy has become a routine procedure in the management of acute abdominal disease and can be a useful therapeutic and additional diagnostic tool in selected cases.6
Red flags that raise suspicion of serious pathology
Hypotension.
Confusion/impaired consciousness.
Signs of shock.
Systemically unwell/septic-looking.
Signs of dehydration.
Rigid abdomen.
Patient lying very still or writhing.
Absent or altered bowel sounds.
Associated testicular pathology.
Marked involuntary guarding/rebound tenderness.
Tenderness to percussion.
History of haematemesis/melaena or evidence of latter on examination per rectum (PR).
Suspicion of a medical cause for abdominal pain.
Special situations
Children
Pain aetiology varies with age; history and examination can be difficult. Please see the separate Abdominal pain in children and Recurrent abdominal pain in children articles.
Pregnancy
Always consider ectopic pregnancy in women of childbearing age. Causes of acute abdomen in late pregnancy are different and require expert combined obstetric, gynaecological and surgical evaluation. Please see the separate Abdominal pain in pregnancy article.
Older patients
Tend to show less specific symptoms and signs.
Tend to present later in the course of their illness.7
Morbidity and mortality in older patients presenting with acute abdominal pain are high.7
You should have a lower threshold for referral to secondary care/for surgical assessment, and a higher index of suspicion of serious pathology.
Aortic aneurysm and bowel ischaemia are more prevalent in the elderly.
Angiodysplasia of the colon is more common and can cause GI haemorrhage.
Medical causes of abdominal pain are encountered more frequently.
The 'Top 5' medical causes of an acute abdomen to consider in older patients are:
Inferior myocardial infarction.
Lower-lobe pneumonia/pulmonary embolism causing pleurisy.
Diabetic ketoacidosis or hyperosmolar nonketotic coma (HONK).
Inflammatory bowel disease (Crohn's disease or ulcerative colitis).
Biliary tract disease, including cholecystitis, is the most common indication for surgery in older patients with abdominal pain. This is thought to be due to age-related changes in the biliary tract.7
Medicolegal pitfalls and tips
Careful documentation of the clinical situation and decision-making process is essential.
Failure to appreciate the severity of illness through not assessing vital signs/taking heed of general condition.
Failing to take note of history from carers/parents in a patient who now seems relatively well, particularly in children.
Failure to examine adequately or to document findings.
Failure to examine for an enlarged bladder, for herniae or to check the scrotum.
Failure to carry out rectal or vaginal examination when it is indicated.
Failing to explain the reason for an intimate examination, leading to an accusation of impropriety.
Treating children as little adults and not considering paediatric-specific diagnoses.
Failing to make concrete follow-up arrangements or advising a patient of when they should seek further assessment, when managing patients in the community.
Delayed transfer of acutely unwell patients to hospital. Use the 999/112/911 service where necessary.
Steroids or other forms of immunocompromise may mask symptoms and signs.
When pain outstrips signs, consider gut infarction or abdominal aortic aneurysm.
Don't rely on a normal test result to discount pathology if the clinical condition suggests otherwise.
Failing to consider pregnancy or conduct a pregnancy test.
Be ready to reassess your initial diagnosis, or a colleague's diagnosis, where the clinical situation has changed.
Exclusive updates for healthcare professionals
Stay informed with the latest clinical updates, professional insights, and evidence-based guidance. The Patient Pro newsletter curates essential content for healthcare professionals—delivered straight to your inbox.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
Further reading and references
- Yang WC, Chen CY, Wu HP; Etiology of non-traumatic acute abdomen in pediatric emergency departments. World J Clin Cases. 2013 Dec 16;1(9):276-84. doi: 10.12998/wjcc.v1.i9.276.
- van Heurn LW, Pakarinen MP, Wester T; Contemporary management of abdominal surgical emergencies in infants and children. Br J Surg. 2014 Jan;101(1):e24-33. doi: 10.1002/bjs.9335. Epub 2013 Nov 29.
- Ranji SR, Goldman LE, Simel DL, et al; Do opiates affect the clinical evaluation of patients with acute abdominal pain? JAMA. 2006 Oct 11;296(14):1764-74.
- Gallagher EJ, Esses D, Lee C, et al; Randomized clinical trial of morphine in acute abdominal pain. Ann Emerg Med. 2006 Aug;48(2):150-60, 160.e1-4.
- Manterola C, Vial M, Moraga J, et al; Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD005660. doi: 10.1002/14651858.CD005660.pub3.
- Navez B, Navez J; Laparoscopy in the acute abdomen. Best Pract Res Clin Gastroenterol. 2014 Feb;28(1):3-17. doi: 10.1016/j.bpg.2013.11.006. Epub 2013 Dec 4.
- Lyon C, Clark DC; Diagnosis of acute abdominal pain in older patients. Am Fam Physician. 2006 Nov 1;74(9):1537-44.
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 17 Jun 2027
18 Jun 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
More in history and examination
- Breast lumps and breast examination
- Femoral nerve lesion
- Flashes, floaters and haloes
- Gradual loss of vision
- Hearing testing and screening in young children
- Heart auscultation
- Hip pain in children
- Horner's syndrome
- Narrow complex tachycardias
- Nasal discharge
- Neonatal jaundice
- Otalgia
- Paediatric examination
- Paediatric supraventricular tachycardia
- Painful foot
- Pierre Robin sequence
- Raynaud's disease
- Rheumatological history, examination and investigations
- Severe and partial sight impairment
- Six-week baby check