Constipation in children
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 26 Sept 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Constipation is a very common problem for children. For most children, constipation means passing hard stools (faeces), with difficulty, less often than normal. Regular soiling (often mistaken for runny diarrhoea) may indicate that a child has bad constipation causing a blockage of the lower part of the gut (impaction). Where no particular disease or illness is the cause of the constipation, it is called idiopathic constipation. It is important that constipation be recognised early to prevent it from becoming a long-term (chronic) problem.
Note: for adults, see the separate leaflet called Constipation.
At a glance
Constipation in children involves straining, pain when passing stools, or passing stools less often than usual.
Stools may be hard, large, or like small pellets.
Other symptoms can include tummy ache, poor appetite, nausea, and irritability.
Common causes include diet (not enough fibre or fluids), stool holding, and emotional factors.
Treatment often involves laxatives, and dietary changes are important for prevention.
See a doctor if you notice vomiting, weight loss, severe pain, or a baby not passing first stool within 48 hours.
What are the symptoms of constipation in children?
Symptoms of constipation in children or babies can mean any, or all, of the following:
Difficulty or straining when passing stools.
Pain when passing stools, sometimes with a tiny amount of blood in the nappy or on the toilet paper, due to a small tear in the skin of the back passage (anus).
Passing stools less often than normal. Generally, this is less than three complete (proper) stools per week.
Stools that are hard and perhaps very large, or pellet-like and small, like rabbit droppings.
As well as less frequent, hard (and perhaps painful) stools, constipation can cause:
Tummy ache (abdominal pain).
Poor appetite.
Feeling 'off colour' (general malaise).
Behavioural changes, such as being more irritable or unhappy.
Fidgeting, restlessness and other signs that the child needs to go to the toilet.
Feeling sick (nausea).
Severe constipation can cause impaction, where a very large stool is stuck in the lower gut, usually just above the anus, in the section called the rectum. This can cause further symptoms. In particular, this can cause a child to soil their pants regularly with very soft faeces, or with faecal-stained mucus. This is often mistaken by parents as diarrhoea. Impaction is discussed in detail later.
What causes constipation in children?
It is thought that various factors may contribute to constipation developing, or may make it worse. These include diet, stool (faeces) holding and emotional factors.
Diet
Dietary factors that may play a part in constipation are:
Not eating enough foods with fibre (the roughage part of the food that is not digested and stays in the gut).
Not having enough to drink.
Stools tend to become harder, drier, and more difficult to pass if there is little fibre and fluid in the gut.
Stool holding or withholding behaviour
This means the child has the feeling of needing the toilet but resists it. The child holds on to the stool, trying to ignore the desire to empty the bowels. This is quite common. You may see your child crossing their legs, sitting on the back of the heels, or doing similar things to help resist the feeling of needing the toilet.
Your child may clench his or her buttocks to try to stop the stool from coming out and may seem quite fidgety. Sometimes it seems as though your child is straining to poo, whereas in fact they are straining to hold it in.
You may notice smudges of stool on your child's pants, often when they are unable to hold on any longer. The longer the child holds on, the bigger the stool gets. Eventually the child has to go but the large stool is more difficult to pass and often more painful. This may lead to a bit of a vicious cycle where the child is even more reluctant to open his or her bowels the next time.
There are a number of reasons why children may hold on to stools:
A previous stool that they passed may have been a struggle or painful. So, they try to put off doing it again.
Their back passage (anus) may be sore or have a crack (anal fissure) from passing a previous large stool. It is then painful to pass further stools. So, the child may resist the urge to pass a stool.
They may have a dislike of unfamiliar or smelly toilets, such as at school or on holiday. The child may want to put things off until they get home.
Emotional problems
Constipation problems may be made worse with upset due to change in surroundings or routine. Common examples are moving house and starting nursery. Potty training may be a factor if a child becomes scared of using the potty. Fears and phobias are usually the underlying reasons for these problems.
What is the treatment for constipation in children?
(Note: this section refers to treatment of idiopathic constipation - the most common type of constipation in children, where there is no known cause. Other types of constipation are explained later.)
How to treat constipation in children
Laxatives
Idiopathic constipation that has lasted for more than a few days is usually treated with laxatives. Your doctor will advise on the type and strength needed. This may depend on factors such as the age of the child, the severity of the constipation and the response to the treatment. Laxatives for children commonly come either as sachets or a powder that is made up into a drink, or as liquid/syrup. The laxatives used for children are broadly divided into two types.
Macrogols (also called polyethylene glycols) are a type of laxative that pulls fluid into the bowel, keeping the stools (faeces) soft. They are also known as osmotic laxatives. For example, Movicol® Paediatric Plain is one brand that is commonly used first. This is mixed into water to make a drink to which cordial, such as blackcurrant squash, can be added to make it taste nicer. Lactulose is another type of osmotic laxative, acting as a stool softener.
Stimulant laxatives. These encourage (stimulate) the bowel to pass the stools out. There are several different types of stimulant laxative. Sodium picosulfate, bisacodyl, senna and docusate sodium are all examples. Docusate works as a stool softener as well as a stimulant. A stimulant laxative tends to be added in addition to a macrogol if the macrogol is not sufficient on its own.
Laxatives are normally continued for several weeks after the constipation has eased and a regular bowel habit has been established. This is called maintenance treatment. So, in total, the duration of treatment may be for several months. Do not stop the prescribed laxatives abruptly.
Stopping laxatives abruptly might cause the constipation to quickly recur. Your doctor will normally advise a gradual reduction in the dose over a period of time, depending on how the stools have become in their consistency and frequency. Some children may even require treatment with laxatives for several years.
Treatment of impaction - if needed
Similar treatments to those listed above are used. The main difference is that higher doses of laxatives are needed initially to clear the large amount of faeces blocking the last part of the bowel (the rectum).
Secondly, laxatives are also usually needed for much longer, as maintenance treatment. The aim is to prevent a build-up of hard stools recurring again, which will prevent impaction returning. The enlarged rectum can gradually get back to a normal size and function properly again.
If laxatives are stopped too soon, a large stool is likely to recur again in the weakened 'floppy' rectum which has not had time to get back to a normal size and strength.
Treatment to clear impacted stools from the rectum can be a difficult time for you and your child. It is likely that your child will actually have a few more tummy pains than before and that there will be more soiled pants. It is important to persevere, as these problems are only temporary. Clearing the impacted stools is an essential part of treatment.
In rare instances, where treatment of impacted stools has failed, a child may be treated in hospital. In hospital, stronger medicines to empty the bowel, called enemas, can be given via the rectum. For very hard to treat cases, a child can have a general anaesthetic and the bowel can be cleared out manually by a surgeon.
Diet
Dietary measures should not be used on their own to treat idiopathic constipation, as it will be unlikely to solve the problem. However, it is still important to get a child into a habit of eating a good balanced diet. This is to include plenty of drinks (mainly water) and foods with fibre. This will help to prevent a recurrence of constipation once it has cleared.
Does my child need any tests?
Tests are not normally needed to diagnose idiopathic constipation. Your GP is likely to ask various questions and do a general examination to rule out secondary causes of constipation.
By examining your child's tummy (abdomen), a GP can tell if there are lots of stools (faeces) in the bowel. This can give an indication if blockage (impaction - discussed later) has developed. If an underlying cause of constipation is suspected, your GP will refer your child to a children's doctor (a paediatrician) and further tests may be done.
How to prevent constipation in children
You can help prevent constipation in your child by making sure they are eating foods with plenty of fibre and drinking plenty. This makes stools (faeces) that are bulky soft and easy to pass out. Getting plenty of exercise is also thought to help.
Food and fibre
This advice applies to babies who are weaned and to children. Foods which are high in fibre are fruit, vegetables, cereals and wholemeal bread. A change to a high-fibre diet is often 'easier said than done', as many children are fussy eaters. However, any change is better than none. Listed below are some ideas to try to increase your child's fibre intake:
A meal of jacket potatoes with baked beans, or vegetable soup with bread.
Dried (or semi-dried) apricots or raisins for snacks.
Porridge or other high-fibre cereals (such as Weetabix®, Shredded Wheat® or All Bran®) for breakfast.
Offer fruit with every meal - perhaps cut up into little chunks to make it look more appealing.
Add extra vegetables to dishes being blitzed with a blender or food processor (for example, Bolognese sauces or soups.
Use wholemeal/brown versions of bread, pasta and rice.
Add powdered bran to yoghurt. The yoghurt will feel grainy, but powdered bran is tasteless.
The Association of UK Dietitians recommends normal daily fibre intake (from the age of 2 years) should be as follows:
Age 2-5: 15 g fibre per day.
Age 6-11: 20 g fibre per day.
Age 12-15: 25 g fibre per day.
Age 16+: 30 g fibre per day.
If you aim for a healthy balanced diet, using wholemeal versions of carbohydrates and 5 portions of fruit/vegetables per day, you should achieve this without having to count.
Drink
If a bottle-fed baby has a tendency to become constipated, you can try offering water between feeds. (Never dilute infant formula milk that is given to bottle-fed babies.) Although it is unusual for a breast-fed baby to become constipated, you can also offer water between feeds.
Older, weaned babies can be given diluted fruit juice (preferably without added sugar). Puréed fruit and vegetables are the usual starting points for weaning, after baby rice, and these are good for preventing constipation.
Encourage children to drink plenty. However, some children get into the habit of only drinking squash, fizzy drinks or milk to quench their thirst. These may fill them up and make them less likely to eat proper meals with food that contains plenty of fibre.
Try to limit these kinds of drinks. Give water as the main drink. However, fruit juices that contain fructose or sorbitol have a laxative action (such as prune, pear, or apple juice). These may be useful from time to time (at mealtimes) if the stools become harder than usual and you suspect constipation may be developing.
Toileting tips
Try to get children into a regular toilet habit. After breakfast, before school or nursery, is often best. Try to allow plenty of time so they don't feel rushed.
Toilet training should be relaxed. Talk with your child about what is happening, explain what you are doing when changing nappies or pants so they understand about 'wee' and 'poo'. Explain what the potty is for. Try to avoid getting upset if they have an accident.
Encouraging your child is helpful. Some kind of reward system is sometimes useful in younger children prone to holding on to stools. You could give a small treat, or use stickers or star charts to reinforce the message.
Praise your child for passing a stool in the potty or toilet but do not punish accidents. It is easy to become frustrated with soiled pants or a child who refuses to pass a stool.
Try to keep calm and not make a fuss over the toilet issue. If your child can see that you are stressed or upset, they will pick up on this feeling; the toileting issue can then become even more of a fraught battle. The aim is to be 'matter of fact' and relaxed about it.
Once they move on to sitting on the toilet, make sure this is manageable - steps and training seats are available. Boys may need to be reminded to sit on the toilet every day to do a poo if they have started to stand to do a wee.
Types of constipation in children and babies
Idiopathic constipation. This is common. The word idiopathic means of unknown cause. Various factors may be involved (discussed later) but many children become constipated for no known reason:
Short bouts of constipation. It is common for children and babies to have a bout of mild constipation for a day or so. This may settle quickly, often without the need for medical treatment.
Long-term constipation. In about 1 in 3 children who become constipated, the problem becomes more long-term (persistent). This is also called chronic idiopathic constipation.
Constipation due to an underlying disease or condition. This is uncommon. The constipation is said to be secondary to this other problem. Some examples of conditions and problems that can cause constipation are:
Some neurological conditions.
Rare diseases with abnormal development of the bowel, such as Hirschsprung's disease.
As a side-effect of certain medications that a child has to take for another condition.
Treatment may involve treating the underlying condition (if that is possible) in addition to tackling the constipation. Worrying symptoms or signs that may indicate a secondary cause include the following. These should be mentioned to your GP. It is also possible that some of these symptoms could mean your child is more seriously unwell:
Being sick (vomiting).
Weight loss or failure to gain weight (thrive).
A swollen, stretched tummy.
Severe pain.
A baby who does not pass a first stool (called meconium) within the first 48 hours of life.
Abnormalities of the back passage (anus) - for example, if it is closed over.
Nervous system (neurological) problems such as weak or paralysed legs.
Sores or ulcers near the anus.
Excessive thirst.
Urinary symptoms - such as passing huge volumes of urine, urine that is very dark or painful urination with smelly urine.
Very pale-coloured stools (especially if the urine is very dark too)
What is idiopathic constipation with impaction?
Impaction means that the bowel is, in effect, blocked by a large amount of hard stool (faeces). Idiopathic constipation with impaction most commonly develops in children between the ages of 2 and 4 years; however, older or younger children can be affected. Symptoms and features include:
Recurrent episodes when the child is uncomfortable or distressed trying to pass a stool.
The child soils their pants regularly with very soft faeces, or with faecal-stained mucus. This is often mistaken by parents as diarrhoea.
The child may also become irritable, not eat much, feel sick, have tummy pains from time to time and generally be out of sorts.
A doctor can often feel a backlog of hard, lumpy stools when he or she examines the child's tummy (abdomen).
The diagram below shows how a child may develop impaction, and the symptoms this may cause.
Chronic constipation
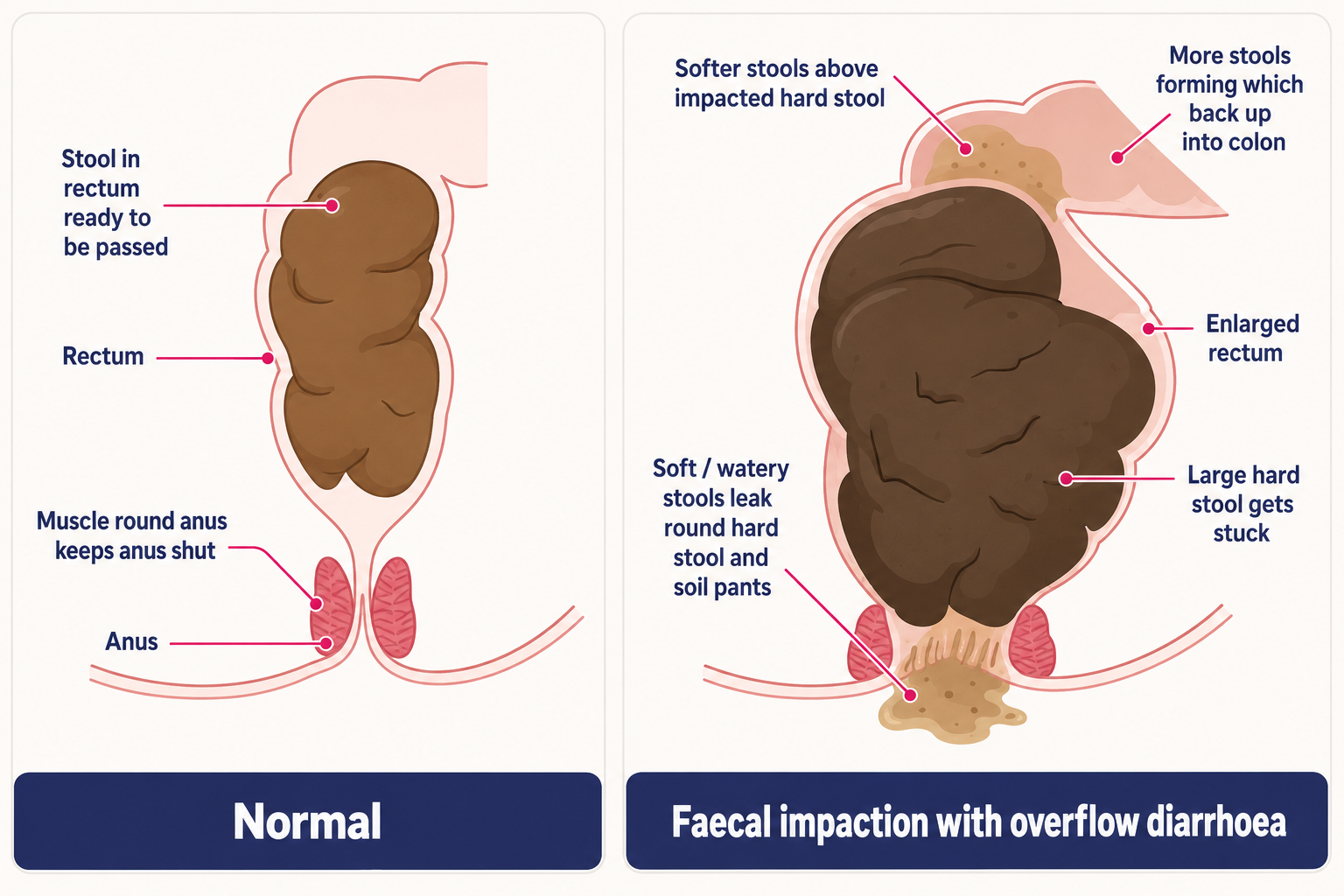
Normally, stools build up in the lowest part of the bowel.
When stools accumulate, they start to pass into the last part of the bowel (the rectum), which stretches. This sends nerve messages to the brain, telling you that you need to empty your bowels.
If the stool is not passed out then more stools from higher up also reach the rectum.
Eventually, large hard stools may build up in the rectum.
The rectum may then stretch and enlarge (dilate) much more than normal, to cope with the excessive amount of stools.
A very large stool may develop and become stuck (impacted) in an enlarged rectum.
If the rectum remains enlarged then the normal sensation of needing the toilet is reduced. The power to pass out a large stool is also reduced (the rectum becomes 'floppy').
More stools build up in the colon behind the impacted stool in the rectum.
The lowest part of an impacted stool lies just above the back passage (anus). Some of this stool becomes runny (liquefies) and leaks out of the anus. This soils the child's pants or bedclothes. Also, some softer, more liquid stools from higher up the colon may bypass around the impacted hard stool. This also leaks out and soils the pants or bedclothes and can be mistaken for diarrhoea. The child has no control of this leaking and soiling.
When a stool is eventually passed, because the rectum is distended and weakened, it simply fills up fairly quickly again with more hard stool from the backlog behind.
For information on constipation affecting adults, see the separate leaflet called Constipation.
Your child's bowels - what is normal?
Parents often become very worried about their child's bowel habit. This anxiety can start when the child is a baby, with concern over the number of dirty nappies. The main thing to realise is that every child is different. Normal can vary quite a bit. Often, it is a change in what is normal for your child that suggests a problem.
Babies will open their bowels anything from several times per day, to once every few days. The frequency of bowel movements is not very important. What is important is that the stools (faeces) are soft and easily passed.
Breast-fed babies tend to pass runnier, mustard yellow-coloured stools. This is because breast milk is better digested than bottle feeds (infant formula). Newborn breast-fed babies may open their bowels with every feed. However, it is also normal for a breast-fed baby to go up to a week without a bowel movement.
Bottle-fed babies often need to open their bowels daily, as the stools are bulkier. Bottle-fed baby stools smell worse (more like an adult's).
It is not uncommon for your baby's stools to vary in colour and consistency from day to day. Any prolonged change to harder, less frequent stools might mean constipation.
As babies are weaned to solid foods, their stools will change in colour and smell. The frequency may again change. Generally, the stools become thicker, darker and a lot more smelly. You will notice that your baby's stools will alter depending upon what you have fed him or her. Some high-fibre foods, such as raisins, may even pass through your baby's bowels virtually unchanged, appearing in the nappy at the next change.
As your baby grows up, into a toddler and then a young child, you may see further changes in their stool frequency and consistency, often dependent on what they are eating.
Your child's bowels - what is abnormal?
As you can see, there is great variation in a child's bowel habit, dependent on their age and what they are fed. As already mentioned, it is often a change in what is normal for your child that suggests a problem. Anything from three times a day to once every other day is common and normal. Less often than every other day means that constipation is likely. However, it can still be normal if the stools (faeces) are soft, well-formed and passed easily.
It may be normal for your baby to go a bit red in the face when straining to pass a stool. This on its own does not necessarily mean they are constipated. Breast-fed babies seldom become constipated, as breast milk contains exactly the right balance of nutrients to keep the stools soft and easily passed.
Diarrhoea usually means very runny stools, often passed more frequently than normal. Breast-fed babies have diarrhoea less frequently than other babies, as breast milk has a protective effect against the germs that can cause diarrhoea.
Patient picks for Digestive conditions

Children's health
Food poisoning in children
Food poisoning occurs when food or water contaminated with harmful germs (microbes), poisons (toxins) or chemicals is eaten or drunk. It usually causes diarrhoea, with or without being sick (vomiting). Sometimes, other problems can be caused by eating contaminated food. In most cases, symptoms clear away over several days but sometimes it takes longer. The main risk of food poisoning is a lack of fluid in the body (dehydration), which can develop more quickly and be more severe in children. The main treatment is to give your child lots to drink to try to avoid dehydration. Any suspected case of food poisoning from eating takeaway or restaurant food should be reported to your local Environmental Health Office. It is important to follow the '4 Cs' to help prevent food poisoning (see below).
by Dr Rosalyn Adleman, MRCGP

Children's health
Toddler's diarrhoea
Toddler's diarrhoea is a common cause of persistent (chronic) diarrhoea in young children. It mainly affects children between the ages of 1 and 5 years and is more common in boys. The child is well in themselves; they have no other symptoms. The diarrhoea will go as the child becomes older. The diet of young children is sometimes thought to contribute to the cause. The diarrhoea will often stop if the child has a good amount of fat in the diet (whole milk, etc), does not drink too much fruit juice or squash and has meals that include a normal amount of fibre (but not a high-fibre diet).
by Dr Philippa Vincent, MRCGP
Frequently asked questions
What is the recommended daily fibre intake for children of different ages?
The Association of UK Dietitians suggests specific daily fibre intakes depending on age. For children aged 2-5, it's 15g per day; for those 6-11, 20g per day; and for 12-15 year olds, 25g per day. Adolescents aged 16 and over should aim for 30g of fibre daily. Achieving a healthy, balanced diet with wholemeal products and five portions of fruit and vegetables per day usually helps meet these targets without needing to count precise amounts.
Are there any drinks that can help with my child's constipation?
While water should be the main drink, certain fruit juices containing fructose or sorbitol, such as prune, pear, or apple juice, have a mild laxative effect. These can be useful if your child's stools become harder than usual and you suspect constipation might be developing. They can be offered occasionally at mealtimes.
What are the early signs that might suggest my child has a more serious underlying health issue causing constipation?
Whilst idiopathic constipation is common, certain symptoms might indicate an underlying condition. These worrying signs include vomiting, weight loss or failure to gain weight, a swollen or stretched tummy, severe pain, or a baby not passing their first stool (meconium) within 48 hours of birth. Abnormalities of the back passage, nervous system problems like weak legs, sores near the anus, excessive thirst, or unusual urinary symptoms (like passing large volumes or discoloured, painful urine) should also be reported to your GP. Very pale stools, especially with dark urine, are also a concern.
What kind of foods are good for increasing my child's fibre intake?
Foods rich in fibre include fruit, vegetables, cereals, and wholemeal bread. You can try serving jacket potatoes with baked beans, or vegetable soup with bread. Dried fruits such as apricots or raisins make good snacks. For breakfast, porridge or high-fibre cereals like Weetabix or Shredded Wheat are good options. Try to include fruit with every meal, perhaps cut into appealing chunks. Extra vegetables can be blended into sauces like Bolognese, or soups. Using wholemeal versions of bread, pasta, and rice can also help. Powdered bran, which is tasteless, can be added to yoghurt.
How can I help my child develop good toilet habits to prevent constipation?
Encourage a regular toilet routine, ideally after breakfast or before school/nursery, allowing plenty of time. Keep toilet training relaxed; talk to your child about what's happening and explain the purpose of the potty. Praise them for passing stools in the toilet or potty, perhaps using a reward system like stickers, but avoid punishing accidents. Try to remain calm and avoid making a fuss, as your stress can make the issue worse for your child. Ensure the toilet is manageable with steps or training seats, and remind boys to sit for bowel movements if they usually stand to wee.
Further reading and references
- Constipation in children and young people; NICE Clinical Guideline (May 2010 - last updated July 2017)
- Bristol Stool Chart
- Fibre; The Association of UK Dietitians (BDA)
- Constipation in children; NICE CKS, August 2025 (UK access only)
- Allen P, Setya A, Lawrence VN; Pediatric Functional Constipation
- Leung AK, Hon KL; Paediatrics: how to manage functional constipation. Drugs Context. 2021 Mar 26;10. pii: dic-2020-11-2. doi: 10.7573/dic.2020-11-2. eCollection 2021.
- Gordon M, MacDonald JK, Parker CE, et al; Osmotic and stimulant laxatives for the management of childhood constipation. Cochrane Database Syst Rev. 2016 Aug 17;(8):CD009118. doi: 10.1002/14651858.CD009118.pub3.
About the authorView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 24 Sept 2028
26 Sept 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in children's health
- Acute diarrhoea in children
- Bedwetting alarms
- Bedwetting medicine - desmopressin
- Bedwetting reward systems
- Breathing difficulties in children
- Childhood obesity
- Club foot
- Congenital heart disease
- Cot death
- Dyslexia
- Head lice treatment and prevention
- Hydrocele in infants
- Immunisation
- Mumps
- Oral thrush in babies
- Pyloric stenosis
- Recurrent abdominal pain in children
- Rubella
- Safeguarding children
- Tear duct blockage in babies