Female sterilisation
Peer reviewed by Dr Hayley Willacy, FRCGP Last updated by Dr Toni Hazell, FRCGPLast updated 19 May 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:SterilisationVasectomy
Female sterilisation is a method of contraception. It is a procedure carried out to prevent eggs from reaching sperm.
At a glance
Female sterilisation is a permanent contraceptive method.
It involves cutting or blocking the Fallopian tubes to prevent eggs from reaching sperm.
The procedure usually takes about 20 minutes and is often done as a day-case.
It is 99.5% effective, meaning 1 in 200 women may become pregnant within a year.
Recovery from a keyhole procedure typically takes a few days.
Sterilisation does not protect against sexually transmitted infections.
If you have pain or unexplained bleeding after sterilisation, see a doctor quickly.

How is female sterilisation done?
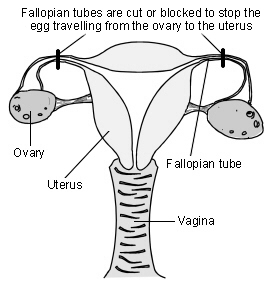
The tubes between the ovary and the womb (the Fallopian tubes) are cut or blocked with rings or clips. This stops the eggs which are released by the ovary from reaching the sperm.
Female reproductive organs
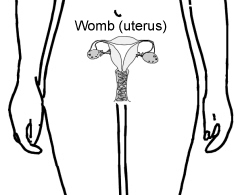
Diagram showing how female sterilisation is performed
The operation is usually done under general anaesthetic but can be done with a local or regional anaesthetic while you are awake. For most women the operation is done with the help of a special telescope called a laparoscope.
The laparoscope is inserted through a very small cut in your tummy (abdomen). It allows the surgeon to see what they are doing. Another small cut is then made to insert an instrument to block the tubes. A number of ways are used to do this. Most often clips or rings are applied to your tubes. The clips or rings provide a block in the tubes and prevent the egg from meeting sperm.
A larger cut may have to be made, and a more traditional operation done, in some women. This is more likely if laparoscopy is too risky, such as if you have had multiple previous operations, or if you are overweight. This is called a mini-laparotomy.
If blocking the Fallopian tubes doesn't work then either part or all of the tubes can be removed. This is called a salpingectomy.
Sterilisation can be performed at the same time as a caesarean section, when a segment of the tube is removed. This is done after the delivery of the baby. It has a higher failure rate than a sterilisation which is not done at the time of caesarean delivery.
How long does the procedure take?
The procedure itself usually takes about 20 minutes, and should be done as a day-case, so you arrive at hospital early in the morning and go home the same day (unless there are unexpected complications).
How reliable is female sterilisation?
The failure rate of female sterilisation is 0.5%, so 1 in 200 women will get pregnant within one year As a comparison, when no contraception is used, more than 800 out of 1,000 sexually active women will become pregnant within one year. This failure rate is much higher than for some long-acting reversible contraceptive (LARC) methods (for example only 1 woman in 2000 will get pregnant per year on the implant) and so a LARC should always be offered to a woman who is considering sterilisation.
After sterilisation, women can become pregnant if the tubes come back together again after being cut. If clips were used to block the tubes, the clips can occasionally work their way off - even when they have been put on correctly.
Advantages of female sterilisation
Do you still have periods after being sterilised?
It is permanent and you (and your partner) don't have to think about contraception again. There are no hormones involved, so you do not have the side-effects of many other types of contraception.
Disadvantages of female sterilisation
Sterilisation is permanent and very difficult to reverse. Some women may regret having the operation in future years, particularly if their circumstances change. Periods may become heavier after sterilisation - sometimes this is because you have stopped using another method, such as the pill, which lightens your periods, but it can also happen if you have not moved from another method.
In the rare event that the procedure fails and you become pregnant, you are more likely to have an ectopic pregnancy. This occurs when the pregnancy develops outside of the womb, usually in the Fallopian tube. You would need emergency treatment if this were to happen. If you think you are pregnant after a sterilisation, or have unexplained bleeding or pain in your tummy (abdomen), then see a doctor quickly.
Laparoscopic sterilisation is also not as easy to do or as effective as male sterilisation (vasectomy). There is a small risk from the insertion of the laparoscope which has to be done 'blind' (ie without any image guidance). This means the surgeon cannot see exactly where they are putting the instrument in the tummy to gain access to the tubes.
It may at times damage organs like bowel or a blood vessel inside the abdomen. This sounds worrying. However, the surgeon takes many precautions to make the procedure safe and to avoid causing damage to any other organ and, in most cases, this does not happen.
Sterilisation doesn't protect against sexually transmitted infection (STIs) so you may need to use condoms if you think you may be at risk of STI.
As with any operation there is a risk of a wound infection and the slight risk from a general anaesthetic. There may be some tummy discomfort or bloating, or mild discomfort or pain at the site of the cut.
How soon is female sterilisation effective?
For laparoscopic sterilisation it depends on when you have it done in your menstrual cycle. If it is done whilst you have your period, you will not have produced an egg yet. In this case the procedure is effective immediately.
At any other time in your cycle, you will usually be advised to continue your previous method of contraception until your next period.
(The procedure is only done after checking you are not pregnant. That is, a pregnancy test would be done. If you have had sex without using contraception in the previous three weeks it is not possible to be sure you will not be pregnant. In this case, the operation would be delayed.)
Does female sterilisation affect sex drive?
No. Sex may seem more enjoyable, as the worry of pregnancy and contraception is removed.
How long does it take to recover from female sterilisation?
It usually takes a few days to recover from a laparoscopic sterilisation and most people can return to work within five days, but should avoid heavy lifting for a week. If a mini-laparotomy (open surgery rather than keyhole) was needed then recovery will be longer, and you may need to be off work for 3-4 weeks and avoid heavy lifting for 6 weeks. It is always important to care for yourself after surgery.
Points to consider
Don't consider having the operation unless you and your partner are sure you do not want children, or further children. It is wise not to make the decision at times of crisis or change - for example, after a new baby or termination of pregnancy. Don't make the decision if there are any major problems in your relationship with your partner. It will not solve any sexual problems.
Doctors normally like to be sure that both partners are happy with the decision before doing this permanent procedure. However, it is not a legal requirement to get your partner's permission. If you have any doubts and questions, make sure you discuss these with your doctor or practice nurse.
Have you considered the alternatives? Female sterilisation is not 100% effective. Other reversible methods of contraception are often more effective, such as the intrauterine system (IUS), contraceptive implants and contraceptive injections. Also, male sterilisation is easier and safer to do and is more effective.
Patient picks for General surgery and procedures

Surgery and procedures
Video-assisted thoracoscopic surgery
Video-assisted thoracoscopic surgery (VATS) is a surgical procedure that allows doctors to see inside the chest and lungs. It is a form of 'keyhole' surgery which can be used to do a number of different surgical procedures. Note: the information below is a general guide only. The arrangements, and the way tests are performed, may vary between different hospitals. Always follow the instructions given by your doctor or local hospital.
by Dr Laurence Knott

Surgery and procedures
Vasectomy
Vasectomy is a a form of birth control where a man undergoes a small operation to cut the end of the vas deferens tube. This is the tube that takes sperm from the testicles (testes) to the penis. Sperm are made in the testes. Once the vas deferens is cut, sperm can no longer get into the semen that comes out (is ejaculated) during sexual intercourse. Vasectomy is very reliable - but not quite 100%. Even after a successful operation about 1 in 2,500 men who have had a vasectomy will become fertile again at some point in the future. This is because, rarely, the two ends of the cut vas deferens re-unite over time.
by Dr Philippa Vincent, MRCGP
Frequently asked questions
What is the advantage of sterilisation compared to other methods of contraception?
The main advantage of female sterilisation is that it is permanent, meaning you and your partner do not have to think about contraception again. Additionally, it involves no hormones, so you avoid the side-effects associated with many other types of hormonal contraception.
Is female sterilisation a completely safe procedure?
While surgeons take many precautions to ensure safety, there are some risks associated with female sterilisation. These include a small risk of damage to organs like the bowel or blood vessels during the insertion of the laparoscope. As with any operation, there's also a risk of wound infection and a slight risk from general anaesthesia. There might be some temporary tummy discomfort, bloating, or pain at the incision site.
Does female sterilisation offer protection against sexually transmitted infections (STIs)?
No, female sterilisation does not protect against sexually transmitted infections. If you believe you may be at risk of STIs, you will still need to use condoms.
Are there any specific situations where the decision to have a sterilisation should be delayed?
It is advised not to make the decision to have a sterilisation during times of crisis or significant life changes, such as after a new baby or a termination of pregnancy. Also, if there are major problems in your relationship, it is recommended to delay the decision. The procedure should not be undertaken with the expectation that it will resolve sexual problems.
Who typically makes the decision for female sterilisation, and is a partner's consent required?
While doctors usually prefer that both partners are in agreement with the decision due to the permanent nature of the procedure, it is not a legal requirement to obtain your partner's permission for female sterilisation.
Further reading and references
- Trussell J; Contraceptive failure in the United States, Contraception, 2011
- Male and female sterilisation; Faculty of Sexual and Reproductive Healthcare (September 2014)
- Contraception - sterilization; NICE CKS, May 2021 (UK access only)
About the authorView full bio

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 12 May 2028
19 May 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in surgery and procedures
- Anaesthetic for hip or knee replacement
- Bone marrow biopsy and aspiration
- Common postoperative complications
- Cystoscopy
- Deep vein thrombosis
- Endobronchial ultrasound-guided transbronchial needle aspiration
- ERCP
- Fever
- Gastroscopy
- Laparoscopy and laparoscopic surgery
- Laser eye surgery
- Lip enhancement
- Local anaesthesia for your eye operation
- Nerve damage after epidural injection
- Post-dural puncture headache
- Preventing infection after splenectomy
- Pulmonary embolism
- Sigmoidoscopy
- Sterilisation
- Video-assisted thoracoscopic surgery