Cervical spondylosis
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Doug McKechnie, MRCGPLast updated 18 Dec 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Neck painWhiplash neck sprainTorticollis
This leaflet is aimed at people who have been told they have cervical spondylosis as a cause of their neck symptoms. Cervical spondylosis is a 'wear and tear' of the vertebrae and discs in the neck. It is a normal part of ageing and does not cause symptoms in many people. However, it is sometimes a cause of neck pain. Symptoms tend to come and go. Treatments include keeping the neck moving, neck exercises and painkillers. In severe cases, the degeneration may cause irritation or pressure on the spinal nerve roots or spinal cord. This can cause arm or leg symptoms (detailed below). In these severe cases, surgery may be an option.
At a glance
Cervical spondylosis is age-related wear and tear of the neck bones and discs.
It often causes no symptoms, but can lead to neck pain.
Symptoms can include pain spreading to the shoulders, stiffness, and headaches.
Painkillers and keeping your neck moving are common treatments.
See a doctor if you develop numbness, weakness, or problems with walking or bladder function.
In this article:
Video picks for Back and spine
Continue reading below
Understanding the neck
The back of the neck includes the cervical spine and the muscles and ligaments that surround and support it. The cervical spine is made up of seven bones called vertebrae. The first two are slightly different to the rest, as they attach the spine to the skull and allow the head to turn from side to side. The lower five cervical vertebrae are roughly cylindrical in shape - a bit like small tin cans - with bony projections.
The sides of the vertebrae are linked by small facet joints. Between each of the vertebrae is a 'disc'. The discs are made of a tough fibrous outer layer and a softer gel-like inner part. The discs act like shock absorbers and allow the spine to be flexible.
Strong ligaments attach to adjacent vertebrae to give extra support and strength. Various muscles attached to the spine enable the spine to bend and move in various ways. (The muscles and most ligaments are not shown in the diagram, for clarity.)
The spinal cord, which contains nervous tissue carrying messages to and from the brain, is protected by the spine. Nerves from the spinal cord come out from between the vertebrae in the neck to take and receive messages to the neck and arms. A major blood vessel called the vertebral artery also runs alongside the vertebrae to carry blood to the rear (posterior) part of the brain.
Cervical spine
Side view of part of the spine
What is cervical spondylosis?
Back to contentsCervical spondylosis is an age-related degeneration ('wear and tear') of the bones (vertebrae) and discs in the neck. To an extent, we all develop some degeneration in the vertebrae and discs as we become older. It tends to start sometime after the age of about 30.
One feature of the degeneration is that the edges of the vertebrae often develop small, rough areas of bone called osteophytes. Also, over many years, the discs become thinner. This degeneration is a normal ageing process which can be likened to having 'wrinkles in the spine'.
In many people, cervical spondylosis does not cause any symptoms. For example, more than 8 out of 10 people over the age of 60 have signs of cervical spondylosis on X-rays or scans, but don't experience any symptoms from it.
However, in some people, the nearby muscles, ligaments, or nerves may become irritated or pressed on by the degenerative changes. So, cervical spondylosis often causes no problems but can be a cause of neck pain, particularly in older people.
Continue reading below
What are the symptoms of cervical spondylosis?
Back to contentsIf symptoms develop, they can range from mild to severe. Symptoms may include:
Pain in the neck:
This may spread to the shoulders and base of the skull. Movement of the neck may make the pain worse.
The pain sometimes spreads down an arm to a hand or fingers. This is caused by irritation of a nerve which goes to the arm from the spinal cord in the neck.
The pain tends to come and go with flare-ups from time to time. You may have a flare-up of pain after unaccustomed use of your neck, or if you sprain a neck muscle or ligament.
However, a flare-up often develops for no apparent reason. Some people develop chronic (persistent) pain.
Some neck stiffness, particularly after a night's rest.
Headaches may occur. The headaches often start at the back of the head just above the neck and travel over the top to the forehead.
You may develop 'pins and needles' in part of an arm or hand. This symptom is caused by irritation of a spinal nerve as it leaves the bony (vertebral) area. However, do tell a doctor if loss of feeling (numbness) or weakness develops in a part of a hand or arm. These symptoms suggest more pressure on a nerve. This is called a 'cervical radiculopathy'.
More rarely, clumsiness of a hand, problems with walking, or problems with bladder function occur when pressure from a worn bone (vertebra) or disc damages the spinal cord. This is called 'cervical myelopathy'. Again, it is important to report these symptoms to a doctor.
Note: cervical radiculopathy and cervical myelopathy are discussed further later in the leaflet. The following section concerns cervical spondylosis without radiculopathy or myelopathy.
Treatments for cervical spondylosis
Back to contentsExercise your neck and keep active
Aim to keep your neck moving as normally as possible. During flare-ups the pain may be quite bad and you may need to rest for a day or so. However, gently exercise the neck as soon as you are able to do so. You should not let it stiffen up. Gradually try to increase the range of the neck movements. Every few hours gently move the neck in each direction. Do this several times a day.
As far as possible, continue with normal activities. You will not cause damage to your neck by moving it.
Medicines
Painkillers are often helpful.
Paracetamol at full strength is often sufficient. For an adult this is two 500 mg tablets, four times a day.
Anti-inflammatory painkillers. Some people find that these work better than paracetamol. They can be used alone or in combination with paracetamol. They include ibuprofen which you can buy at pharmacies or obtain on prescription. Other types such as diclofenac or naproxen need a prescription. Some people with stomach ulcers, asthma, high blood pressure, kidney failure, or heart failure may not be able to take anti-inflammatory painkillers.
A stronger painkiller such as codeine is an option if anti-inflammatories do not suit or do not work well. Codeine is often taken in addition to paracetamol. Constipation is a common side-effect from codeine. To prevent constipation, have lots to drink and eat foods with plenty of fibre.
Medicines to treat nerve pain (neuropathic pain) are sometimes useful in people with persistent (chronic) neck pain. These include:
A low-dose tricyclic antidepressant, such as amitriptyline. The dose of amitriptyline used for pain is 10-30 mg at night. At higher doses, tricyclic antidepressants are used to treat depression. However, at lower doses they have been found to help relieve certain types of pain, including neck pain.
Duloxetine. Duloxetine is a different type of antidepressant. Like amitriptyline, although it was originally developed to treat depression, it can also be useful for treating nerve pain.
Gabapentin or pregabalin. These are medicines that were originally developed to treat epilepsy, but can be useful for treating nerve pain.
Physiotherapy
If symptoms do not improve over a week or so, you may then be referred to a physiotherapist to help with pain relief and for advice on specific neck exercises.
Various treatments may be advised by a physiotherapist. These include traction, heat, cold, manipulation, etc. The value of each of these treatments is uncertain, as the results of research studies looking at which treatments work best can be conflicting.
However, what is often most helpful is the advice a physiotherapist can give on neck exercises to do at home. A common situation is for a doctor to advise on painkillers and gentle neck exercises.
Other treatments
Some other treatments which may be advised include:
A good posture may help. Check that your sitting position at work or at the computer is not poor (that is, not with your head flexed forward with a stooped back). Sit upright. Yoga, Pilates and the Alexander Technique all improve neck posture; however, their value in treating neck pain is uncertain.
A firm supporting pillow seems to help some people when sleeping. Try not to use more than one pillow.
Treatment may vary and you should go back to see a doctor:
If the pain becomes worse or severe.
If other symptoms develop such as loss of feeling (numbness), weakness, or persistent pins and needles in a part of an arm or hand, as described previously.
If you develop any problems with walking or with passing urine. Again these symptoms suggest that cervical myelopathy may be developing as a complication of the cervical spondylosis.
If you develop dizziness or blackouts when turning the head or bending the neck. This can suggest that the vertebral artery which supplies the brain is being nipped by the degenerative changes in the spine.
Other pain-relieving techniques may be tried if the pain becomes chronic. For example, you may be referred to a pain clinic and a pain management programme may be offered to help you control and live with your pain.
Chronic neck pain is also sometimes associated with anxiety and depression which may also need to be treated.
Continue reading below
Cervical radiculopathy and cervical myelopathy
Back to contentsCervical spondylosis is an age-related degeneration ('wear and tear') of the bones (vertebrae) and discs in the neck. Sometimes, it can put pressure on the nerves coming out of the spine (cervical radiculopathy) or on the spine itself (cervical myelopathy). Most cases do not. However, it may be useful to be aware of the symptoms that suggest they may be happening, particularly as some of them may develop slowly. See a doctor if you suspect that you are developing cervical radiculopathy or cervical myelopathy.
Cervical radiculopathy
This occurs when the root of a nerve is pressed on or damaged as it comes out from the spinal cord in the neck (cervical) region. Although there are other causes of radiculopathy, cervical spondylosis is a common cause.
Degenerative changes to the joints around the vertebrae and osteophyte formation produce areas of narrowing which may nip the nerve. Another cause is a prolapsed disc. This is sometimes called a 'slipped disc' although the disc does not actually slip. What happens is that part of the inner softer area of the disc bulges out (prolapses) through a weakness in the outer harder part of the disc. This presses on the nerve as it passes out between the vertebra (see diagram).
Cervical vertebra
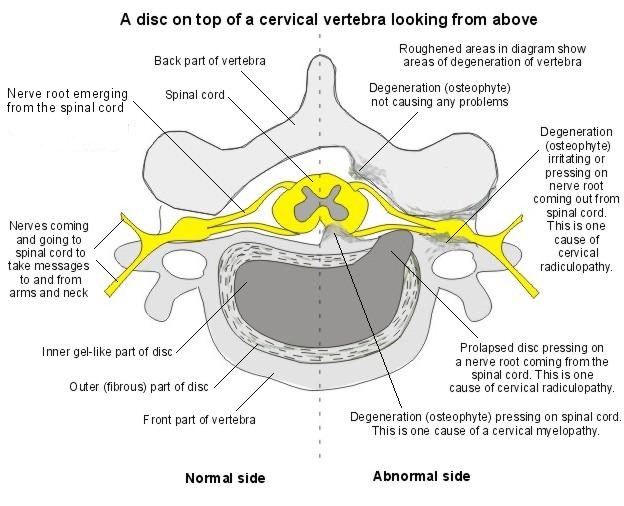
As well as neck pain, symptoms of radiculopathy include loss of feeling (numbness), pins and needles, pain and weakness in parts of an arm or hand supplied by the nerve. These other symptoms may actually be the main symptoms rather than neck pain. There may be shooting pains down into the arm. The symptoms are usually worse in one arm but may affect both. The pain may be severe enough to interfere with sleep. The lower cervical vertebrae are the usual ones affected, causing these symptoms in the arms. However, if the upper vertebrae are involved, the pain and numbness occur at the back and the side of the head.
Your doctor may suspect a radiculopathy if you have the typical symptoms. A doctor's examination may show changes to the sensation, power and tendon reflexes to areas of the arm supplied by the affected nerve. You may then be referred to a specialist for further tests. These may include an MRI scan which will show whether the nerve roots are being pressed on.
Treatment will depend on how severe the pressure and damage are. In many cases the symptoms settle over time. A course of physiotherapy or a neck collar used for a prescribed period may help. However, in some situations, surgery may be recommended which aims to relieve the pressure on the nerve. Depending on the cause, this may involve surgery to the disc or to the vertebra itself.
Cervical myelopathy
This occurs when there is pressure on or damage to the spinal cord itself. Again, cervical spondylosis is a common cause of this condition, as the degenerative changes to the vertebra can narrow the canal through which the spinal cord passes. A prolapse of a cervical disc can also cause myelopathy if the prolapse is into the central canal of the vertebra. This may happen suddenly or develop over a period of time. There are various other rare causes of cervical myelopathy. For example, a tumour or infection that affects this part of the spinal cord.
As the spinal cord is made up of groups of nerve fibres carrying messages to the brain from the rest of the body, pressure on these nerves in the neck region can produce symptoms from several parts of the body.
The symptoms of a cervical myelopathy may include:
Difficulties with walking. For example, the legs may feel stiff and clumsy.
Changes to the sensation of the hands. For example, it may be difficult to feel and recognise objects in the usual way and you may have a tendency to drop things.
Problems with your bladder. For example, you may experience problems with emptying your bladder, or incontinence.
A doctor's examination may show changes to the sensation, power and tendon reflexes to the legs and arms. You are likely to be referred to a specialist for further tests, usually an MRI scan. This will show how the spinal cord is affected and whether any surgical treatment to relieve the pressure is likely to help.
Patient picks for Back and spine

Bones, joints and muscles
Torticollis
Torticollis means 'twisted neck'. It is also often called 'wry neck'.
by Dr Surangi Mendis, MRCGP

Bones, joints and muscles
Whiplash neck sprain
A whiplash neck sprain (also know as just whiplash) is common after a road traffic accident. Symptoms usually ease and go without any specific treatment. It is best to keep the neck active and moving. If required, painkillers can ease pain.
by Dr Doug McKechnie, MRCGP
Frequently asked questions
What is the difference between neck pain from cervical spondylosis and other types of neck pain?
Cervical spondylosis specifically refers to neck pain caused by age-related 'wear and tear' of the bones (vertebrae) and discs in the neck. While many people over 60 show signs of cervical spondylosis on scans without symptoms, it can cause pain if the degenerative changes irritate or press on nearby muscles, ligaments, or nerves. Other neck pains might stem from injuries, muscle strains, or different conditions not related to this specific age-related degeneration.
If I have cervical spondylosis, does that mean I will definitely develop problems like cervical radiculopathy or myelopathy?
No, not necessarily. Cervical spondylosis is an age-related degeneration that affects most people eventually. However, in most cases, it does not lead to cervical radiculopathy (pressure on nerve roots) or cervical myelopathy (pressure on the spinal cord itself). These more severe complications only occur when the degenerative changes become significant enough to put pressure on the nerves or spinal cord.
Can sleeping position or mattress quality affect cervical spondylosis symptoms?
While the article doesn't specifically mention mattress quality, it does suggest that using a firm supporting pillow can help some people when sleeping. It also advises against using more than one pillow. Maintaining good posture, including while sleeping, can be beneficial.
Are there any alternative therapies that can help with cervical spondylosis?
The article mentions that some other treatments might be advised. For improving neck posture, yoga, Pilates, and the Alexander Technique are listed. However, it notes that the value of these specific approaches in treating neck pain is uncertain from a medical standpoint, though they can improve posture.
How long do flare-ups of cervical spondylosis pain typically last?
The article states that cervical spondylosis pain tends to 'come and go with flare-ups from time to time.' It doesn't specify a typical duration for these flare-ups but notes that they can occur after unaccustomed neck use or a sprain, or often for no apparent reason. It also mentions that some people develop chronic (persistent) pain.
When should I see a doctor if my neck pain gets worse or new symptoms appear?
You should go back to see a doctor if your pain becomes worse or severe. Also, seek medical attention if other symptoms develop, such as loss of feeling, weakness, or persistent pins and needles in an arm or hand. Problems with walking or passing urine, or dizziness or blackouts when turning or bending the neck, also warrant immediate medical review, as these can indicate more serious complications like cervical myelopathy or issues with blood supply to the brain.
Further reading and references
- Kuijper B, Tans JT, Beelen A, et al; Cervical collar or physiotherapy versus wait and see policy for recent onset cervical radiculopathy: randomised trial. BMJ. 2009 Oct 7;339:b3883. doi: 10.1136/bmj.b3883.
- Jiang SD, Jiang LS, Dai LY; Degenerative cervical spondylolisthesis: a systematic review. Int Orthop. 2011 Jun;35(6):869-75. doi: 10.1007/s00264-010-1203-5. Epub 2011 Jan 25.
- McCormick JR, Sama AJ, Schiller NC, et al; Cervical Spondylotic Myelopathy: A Guide to Diagnosis and Management. J Am Board Fam Med. 2020 Mar-Apr;33(2):303-313. doi: 10.3122/jabfm.2020.02.190195.
- Neck pain - cervical radiculopathy, NICE CKS, November 2023 (UK access only)
- Neck pain - non-specific; NICE CKS, April 2023 (UK access only)
Continue reading below
About the authorView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 17 Dec 2027
18 Dec 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.