Levonorgestrel intrauterine device
Intrauterine System (IUS)
Peer reviewed by Dr Surangi Mendis, MRCGPLast updated by Dr Toni Hazell, FRCGPLast updated 17 Sept 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Long-acting reversible contraceptivesContraceptive implantContraceptive injectionIntrauterine contraceptive device
The levonorgestrel intrauterine device (LNG-IUD), previously known as the intrauterine system (IUS) is a small, flexible, plastic device which sits inside the womb (uterus). There are two threads attached to it which pass out through the neck of the womb.
At a glance
The levonorgestrel intrauterine device (LNG-IUD) is a very effective contraception method.
It is a small, flexible, plastic device that sits inside the womb and releases hormones.
Some types also treat heavy periods, endometriosis, or are part of hormone replacement therapy.
Depending on the type, it can last for 3, 5, or 8 years.
You may have irregular bleeding for the first 3 to 6 months after fitting.
See a doctor if you have prolonged abdominal pain, vaginal discharge, or cannot feel the threads.

The levonorgestrel intrauterine device (LNG-IUD) is a very effective method of contraception. Some types of LNG-IUD may also be used to treat heavy periods (menorrhagia) and conditions such as endometriosis. The LNG-IUD sits inside the womb (uterus).
Once fitted, it works as a contraceptive, with the length of this effect depending on the dose of the LNG-IUD. If your LNG-IUD has 52mg of hormone in it, guidelines in the UK say that you can use it for contraception for up to 8 years, even though it is only the Mirena® brand that has a licence for this duration. The 19.5mg LNG-IUD can be used for 5 years and the 13.5mg LNG-IUD can be used for up to 3 years. Most women who use a LNG-IUD have no problems with it. It is sometimes called a "hormone coil" because in the 1960s some intrauterine contraceptives were coil-shaped, and because it contains a hormone, levonorgestrel.
What is the levonorgestrel intrauterine device and what does it look like?
What is a LNG-IUD?
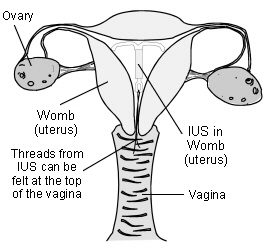
The LNG-IUD is a small, flexible, plastic device which sits inside the womb (uterus). There are two threads attached to it which pass out through the neck of the womb (cervix) and lie in your vagina (see diagram below). These allow you to check it is still there. They also mean it can be removed easily. They do not hang outside the body and your partner should not be able to feel them during sex (intercourse).
Unlike the copper intrauterine device (Cu-IUD), the LNG-IUD does not contain copper; it contains a slow-release progestogen hormone called levonorgestrel (LNG). It is therefore called a levonorgestrel intrauterine device, shortened to LNG-IUD.
What are the different types of LNG-IUD?
Types of levonorgestrel intrauterine device
There are several types of LNG-IUD available. They are all T-shaped (the two side arms fold flat for insertion and fold up for removal) and about the length of a matchstick. The inside of the womb itself is only a little longer than a matchstick, so the LNG-IUD fits neatly inside. The LNG-IUD can be inserted quite easily into a woman's womb by a trained doctor or nurse.
The different types of LNG-IUD vary according to their size and how much hormone they contain.
Mirena® was the first LNG-IUD. It is the largest and contains 52 mg levonorgestrel.
Benilexa® and Levosert® also contain 52 mg levonorgestrel.
Kyleena® is smaller than Mirena® and contains 19.5 mg levonorgestrel.
The LNG-IUD with the least amount of hormone is called Jaydess®. It is the same size as Kyleena® but contains only 13.5 mg levonorgestrel.
The various brands of LNG-IUD have different licences in the UK. Mirena® has a licence for contraception, treating heavy periods, and as part of hormone replacement therapy. Levosert® has a licence for contraception and treating heavy periods. Benilexa®, Kyleena® and Jaydess® only have a licence for contraception. However, UK guidance states that any 52mg LNG-IUD can be used for contraception, heavy periods and as part of hormone replacement therapy, even though this is outside of the licence for some of the brands. Kyleena® and Jaydess® can only be used for contraception, although they may have an incidental effect of making periods lighter.
Note: the various types of LNG-IUD may go by different names in different countries and may not all be available where you live.
How does the levonorgestrel intrauterine device work as a contraceptive?
The LNG-IUD works differently to the Cu-IUD because instead of copper it contains levonorgestrel, a progestogen hormone. The hormone thickens the mucus in the neck of the womb (cervix). This forms a plug which stops sperm getting through to the womb (uterus) to fertilise an egg.
The hormone also this the lining of your womb. So if an egg does fertilise, it is unlikely to implant. Also, it makes your periods much lighter, or they may disappear altogether.
In some women the LNG-IUD prevents an egg being released as well, so that it happens less often or not at all. However, this is usually not the case, even if your periods are absent when using the LNG-IUD, particularly with the lower-dose LNG-IUD.
How effective is the levonorgestrel intrauterine device for contraception?
The LNG-IUD is extremely effective. Around 2 in 1,000 women using the LNG-IUD will become pregnant each year. Compare this with rates of pregnancy when no contraception is used. More than 800 in 1,000 sexually active women who do not use contraception become pregnant within one year. This figure rises to 950 in two years.
Why would I choose a levonorgestrel intrauterine device?
Effective contraception
Once a LNG-IUD is inserted you no longer need to use other contraception for between three and eight years. So, unlike users of the contraceptive pill, you do not have to think about contraception every day.
The LNG-IUD does not interfere with having sex (intercourse) or with sex drive (libido). Although it contains progestogen, the quantity of the hormone which gets into your general system is very low. It does not usually therefore cause the side-effects which can occur with higher doses of hormones (for example, in progestogen-only injectable contraceptives).
Period problems improve
Periods usually become lighter, less painful and often stop, unlike with the copper IUD. After 12 months most users only have a light bleed for one day per month or so, and about 1 in 5 users of the 52mg LNG-IUD have no bleeding at all. This is why a LNG-IUD can be so good at treating heavy periods (menorrhagia), painful periods (dysmenorrhoea) and endometriosis.
Easily reversible
Fertility returns as soon as the LNG-IUD is removed.
Other uses and benefits
The 52 mg LNG-IUD does not have to be used as contraception. It can also be used as a treatment for heavy periods, endometriosis and fibroids, even if you don't need contraception. The LNG-IUD that contain less hormone (Jaydess® and Kyleena®) are not suitable to treat these conditions.
What are the side-effects of the levonorgestrel intrauterine device?
Although the majority of women with a LNG-IUD have no problems, the following may occur:
Irregular bleeding
You may have irregular bleeding for the first three to six months. This usually settles down. It is usually a light "spotting" of blood which women can find a nuisance.
Heavier bleeding can occasionally occur. If you experience heavy bleeding or a marked change in bleeding pattern you should discuss this with your doctor. It may mean the LNG-IUD has come out without you realising, or could be a sign of infection or pregnancy.
Ectopic pregnancy
A pregnancy developing outside the womb (uterus), usually in the Fallopian tube, is known as an ectopic pregnancy and is very unusual with the LNG-IUD. This is because the LNG-IUD protects against this sort of pregnancy. However, if you do develop one-sided tummy (abdominal) pain with bleeding you should do a pregnancy test and discuss this with a doctor.
Expulsion
The LNG-IUD may come out without you noticing (expulsion). This happens to 1 woman in every 20. It usually happens in the first year, particularly in the first three months, during your period. It seems it is slightly more likely to happen if it has happened to you before.
It is a good idea to check you can feel the threads of the LNG-IUD after your period (or once a month if your periods stop). If you cannot feel them, you should use extra precautions such as a condom, until your doctor or nurse has checked the LNG-IUD is still there.
If the LNG-IUD has come out in the previous few days you may need emergency contraception. If the LNG-IUD could have come out more than a few days previously, and you are sexually active, the doctor or nurse will need to make sure you are not already pregnant before fitting another one or starting alternative contraception.
Damage to the womb
The fitting of a LNG-IUD can (very rarely) make a small hole in the womb - this is called perforation. It protrudes through the wall of the womb and can escape into your pelvis. This happens in fewer than 2 per 1,000 women, usually at the time of fitting.
It can cause pain, but this is not usually severe and often there is no pain. The main symptom is not being able to feel the threads. Your womb will heal on its own but you may need an operation to remove the LNG-IUD from your pelvis. The risk of perforation is higher in women who are breastfeeding. Even less commonly (about ten times less common than perforation on its own) is damage to the bladder or bowel, which may need an operation to fix.
You should tell your doctor or nurse if you can no longer feel the threads of your LNG-IUD This may mean perforation has occurred. However, far more commonly it means that the threads are tucked up inside the neck of the womb (cervix). Rarely, it can be because the threads have come off the LNG-IUD. An ultrasound scan will be carried out to find a lost LNG-IUD. If ultrasound does not find the LNG-IUD, an X-ray will be ordered. If neither of these find the LNG-IUD then it can be concluded that it has fallen out.
Hormonal side-effects
Hormonal side-effects are uncommon. The progestogen released by the LNG-IUD mainly stays around the womb and very little gets into the bloodstream. So hormone side-effects are less common than with the progestogen-only pill and the contraceptive injection or implant.
If side-effects do occur, they tend to develop in the first few months. They then tend to ease and go. Examples of possible side-effects include:
Mood swings.
Reduced sex drive (libido).
Fluid retention.
Increase in acne.
Breast discomfort.
A slight increase in breast size - this can occur in the first few months but is usually temporary.
There is no evidence that the LNG-IUD causes women to gain weight.
The LNG-IUD does not protect you against any sexually transmitted infections (STIs); only condom use does that.
Who cannot use the levonorgestrel intrauterine device?
The IUS cannot be used as emergency contraception. If you think you need emergency contraception contact your health professional as soon as you can; you can then be fitted with a copper intrauterine device (Cu-IUD) or be given emergency contraceptive pills. See our reference in Further Reading below to find a sexual health clinic.
Your doctor or family planning nurse will discuss your medical history and will need to ask you some personal questions about your sex life. You may need to have tests done to look for STIs, such as chlamydia and gonorrhoea, but you will probably still be able to have an LNG-IUD fitted while you are waiting for the results, unless you have symptoms.
If you have recently been pregnant, it is recommended that you wait four weeks to have your LNG-IUD fitted (although it can safely be fitted at the time of an abortion or within 48 hours of the birth of a baby, but it may be slightly more likely to come out).
Some illnesses may mean you cannot start to use progestogen-based contraceptives, such as the LNG-IUD. Some of these are relative contraindications, meaning that the decision to use a LNG-IUD or not would be taken after a discussion between you and your doctor. These include:
An infection which has not been treated.
A history of breast cancer.
Current cancer of the lining of the womb (endometrial cancer).
Cancer of the neck of the womb (cervical cancer).
Very large fibroids.
HIV, where your white cell count is very low.
If you have heart disease a cardiologist should be consulted before you have a LNG-IUD fitted and it may be recommended that this is done in hospital.
In practice, the number of women who cannot have the LNG-IUD inserted is small.
How is the levonorgestrel intrauterine device fitted?
This is usually done towards the end of a period or shortly afterwards, as this tends to be more comfortable for you. Also, the doctor can be sure that you are not pregnant. However, it can be fitted at any time provided that you are certain you are not pregnant. You will need to have a vaginal examination.
The doctor or nurse will pass a small instrument into your womb (uterus) to check its size and position. A clip is put on to the neck of your womb (cervix) and the inside of your uterus is measured. The LNG-IUD is then fitted using a small plastic insertion device.
You will be taught how to feel the threads of the LNG-IUD so you can check it is in place. It is best to check the threads regularly - for example, once a month just after a period.
LNG-IUD in place
The procedure can be painful, like an intense period cramp, but the pain usually lasts only a minute or two. After the LNG-IUD is fitted, some women have crampy pains like period pains for a few hours. These can be eased by painkillers such as paracetamol or ibuprofen. Light vaginal bleeding may also occur for a short while.
The Jaydess® and Kyleena® LNG-IUD are narrower than a 52 mg LNG-IUD. This may make them easier and less painful to have fitted.
Does the levonorgestrel intrauterine device work straightaway?
If the LNG-IUD is fitted within five days after the start of a period, it is immediately effective as a contraceptive. If it is fitted after the fifth day then you need to use extra protection such as condoms, or avoid having sex, for seven days.
Note: the LNG-IUD is not effective as emergency contraception.
Do I need any follow-up?
There is no need for a routine follow-up after having a LNG-IUD, as long as you have no worrying symptoms and can feel the threads. If you cannot feel the threads, or you have symptoms such as bad pelvic pain, a smelly discharge, or a temperature, then you should see your doctor urgently.
Most women have no problems and the LNG-IUD can remain in place for up to eight years, depending on the device fitted. If you are 45 years or over at the time of fitting a 52mg device, it can safely be left in place (and will remain effective for contraception) until your menopause, even if this is more than eight years. However, if you are also using it as part of hormone replacement therapy, it must be changed every five years, whatever your age.
If you are using it only to treat heavy periods, and not for contraception or as part of hormone replacement therapy, you can keep it in place for as long as it continues to be effective (although generally it is removed once you are 55).
Removing and changing the levonorgestrel intrauterine device
The LNG-IUD can be removed at any time by a trained doctor or nurse.
You will be able to get pregnant as soon as it is removed. If you plan to have it removed, but do not want to get pregnant, use other methods of contraception (such as condoms) from seven days before it is removed. This is because sperm can last up to seven days after you have had sex (intercourse) and can fertilise an egg AFTER the LNG-IUD is removed.
If you have had your LNG-IUD for its maximum effective time, it will need to be changed. You will need to use other forms of contraception from seven days before it is removed. This is because occasionally when the LNG-IUD is removed the neck of your womb (cervix) clamps tightly shut for a while and a new one cannot be fitted straight away. As sperm can last up to seven days in the womb (uterus) they could therefore fertilise an egg whilst you are waiting for your replacement LNG-IUD fitting.
You can use sanitary towels, tampons or a Mooncup® (menstrual cup) for your period with a LNG-IUD in place. A cervical smear can also be taken with a LNG-IUD in place. Sometimes, the smear result may show that there is an organism in the cervix; these are called actinomyces-like organisms (ALOs).
These are normal and do not mean that the LNG-IUD should be removed. However, if you have had pelvic pain together with signs of infection, such as a temperature, your doctor may consider removing the LNG-IUD. ALOs are much less commonly seen now than in the past, due to changes in the way that smear test samples are processed.
You should consult a doctor if any of the following occur
Prolonged tummy (abdominal) pain after a LNG-IUD is inserted.
Vaginal discharge with or without pain. This may indicate infection.
You can't feel your threads and suspect that the LNG-IUD has come out or is coming out. If you cannot feel the threads or feel something that feels like the head of a match, then use other contraception (such as condoms or not having sex) until you have been checked by a doctor or nurse.
Dr Mary Lowth is an author or the original author of this leaflet.
Patient picks for Contraception

Sexual health
Signs you're on the wrong contraceptive pill
The contraceptive pill often gets a bad rap for its host of potential side effects, which can range from the mildly inconvenient to the downright debilitating. However, it's worth noting that there are around 30 different types of contraceptive pill currently available in the UK, and not all pills are created equal.
by Sarah Graham
Sexual health
Contraception barrier methods
Barrier methods are one group of options for contraception. Condoms are the most well-known type of barrier method. This leaflet signposts towards more information about these and the other barrier methods.
by Dr Mary Harding, MRCGP
Frequently asked questions
Can I use tampons or a menstrual cup with the LNG-IUD?
Yes, you can use sanitary towels, tampons, or a menstrual cup (like a Mooncup®) for your period while you have an LNG-IUD in place.
Does having an LNG-IUD mean I can't have a cervical smear test?
No, a cervical smear test can still be taken with an LNG-IUD in place. Sometimes, the test may show actinomyces-like organisms (ALOs) in the cervix. These are normal and do not usually mean the LNG-IUD needs to be removed, unless you also have pelvic pain and signs of infection.
What should I do if I can't feel the threads of my LNG-IUD?
If you cannot feel the threads of your LNG-IUD, you should use extra contraception, such as condoms, or avoid having sex, until you have seen a doctor or nurse. This is important because it could mean the device has moved, fallen out, or rarely, that it has perforated the womb.
How soon after giving birth can I have an LNG-IUD fitted?
It is recommended to wait four weeks after giving birth to have an LNG-IUD fitted. However, it can safely be fitted at the time of an abortion or within 48 hours of a baby's birth, though there might be a slightly higher chance of it coming out if fitted so soon after delivery.
How long does a 52mg LNG-IUD last if I'm over 45?
If you are 45 years or older when a 52mg LNG-IUD is fitted, it can safely remain in place for contraception until your menopause, even if this period extends beyond the typical eight-year guideline for the device. However, if you are also using it as part of hormone replacement therapy, it must be changed every five years.
Further reading and references
- Long-acting reversible contraception; NICE Clinical Guideline (October 2005 - updated July 2019)
- Trussell J; Contraceptive failure in the United States, Contraception, 2011
- Intrauterine Contraception; Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit (March 2023 - last updated July 2023)
- UK Medical Eligibility Criteria Summary Table for intrauterine and hormonal contraception; Faculty of Sexual and Reproductive Healthcare, 2016 - amended September 2019
- Find a sexual health clinic near you; NHS services
- Contraception - Progestogen-only methods; NICE CKS, November 2024 (UK access only)
- The Hormonal Coil; Brook
About the authorView full bio

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Surangi Mendis, MRCGP
Consultant and Medical Author
MBBS, BSc (1st), MRCGP (2014), DFSRH, PGcert otology and audiology
Surangi Mendis is a consultant in Audiovestibular Medicine and Neuro-otology at The Royal National ENT and Eastman Dental Hospitals, UCLH.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 16 Sept 2027
17 Sept 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in sexual health
- Balanitis
- Contraception barrier methods
- Contraceptive hormone pills, patches and rings
- Dyspareunia
- Emergency contraception
- Epilepsy and contraception
- Erectile dysfunction
- Female sexual dysfunction
- Genital herpes
- Genital warts
- Hypersexuality
- Klinefelter's syndrome
- Progestogen-only contraceptive pill
- Refer yourself to NHS sexual health services
- Sexual assault
- Signs you're on the wrong contraceptive pill
- Sperm test
- STI tests
- Vaginal dryness
- Vasectomy