Urine infection in children
Peer reviewed by Dr Krishna Vakharia, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 26 Aug 2022
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Urine infection in children is common. It can cause various symptoms. A course of medicines called antibiotics will usually clear the infection quickly. In most cases, a child with a urine infection will make a full recovery. Sometimes tests to check on the kidneys and/or bladder are advised after the infection has cleared. Your doctor will advise if your child needs these tests. This depends on your child's age, the severity of the infection and whether it has happened before.
At a glance
A urine infection in children is caused by germs that get into the urine.
Symptoms in young children include fever, vomiting, drowsiness, or appearing unwell.
Older children may have painful or frequent urination, or tummy/back pain.
A urine sample confirms the diagnosis, and antibiotics usually clear the infection.
Give the child plenty to drink and paracetamol for pain or fever.
Seek medical help if you suspect your child has a urine infection.
Prevent future infections by preventing constipation and ensuring good hygiene.
What is a urine infection in children?
The urinary tract
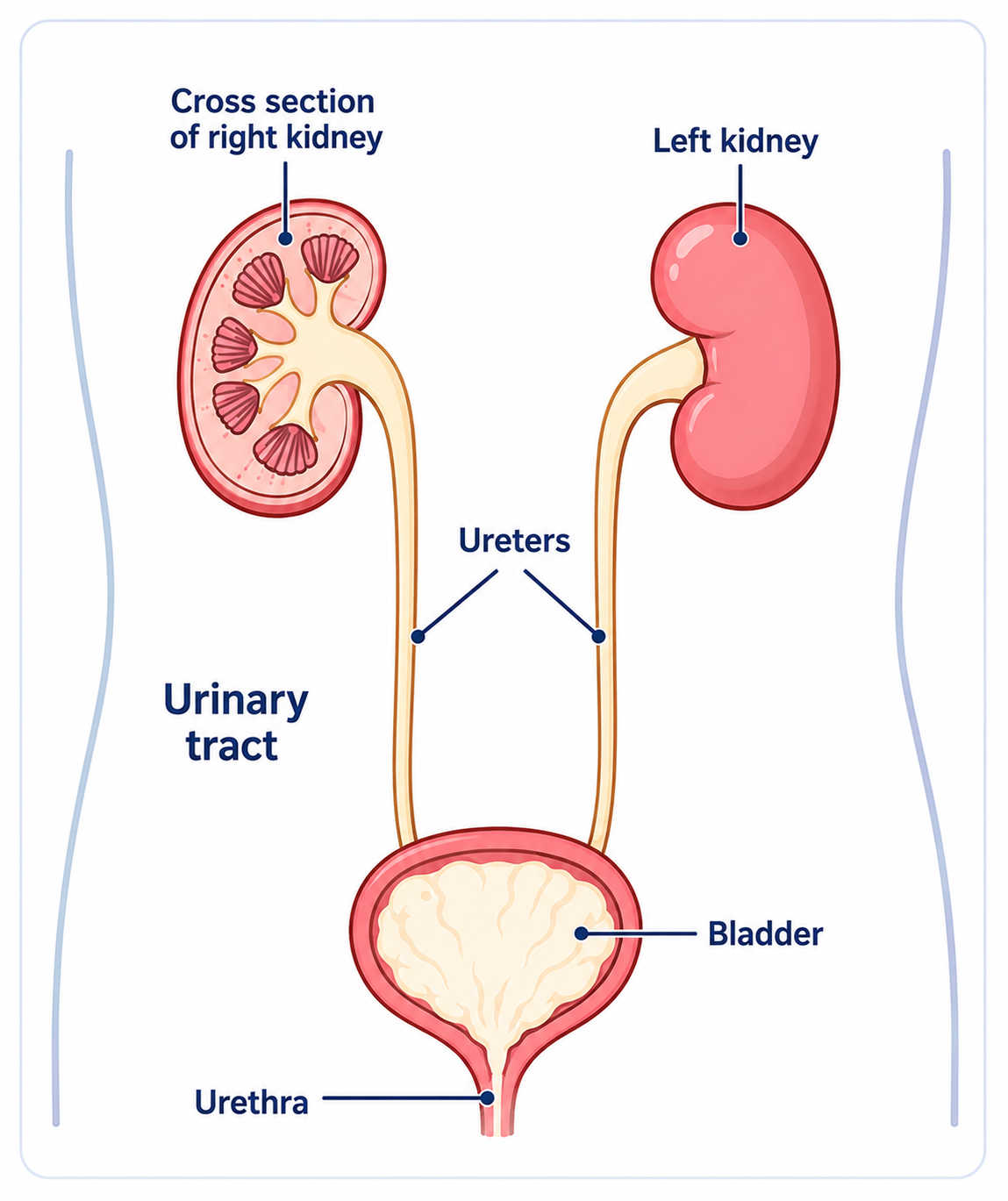
A urine infection is caused by germs (bacteria) that get into the urine. Most urine infections are due to bacteria that normally live in the bowel. They cause no harm in the bowel but can cause infection if they get into other parts of the body. Some bacteria lie around the back passage (anus) after a stool (faeces) has been passed. These bacteria can sometimes travel to the urethra (the tube that passes urine from the bladder) and into the bladder. Some bacteria thrive in urine and multiply quickly to cause infection.
The infection is commonly just in the bladder (when it is called cystitis) but may travel higher up to affect one or both kidneys as well.
Understanding the urinary tract
There are two kidneys, one on each side of the abdomen. They make urine which drains down tubes called ureters into the bladder. Urine is stored in the bladder and is passed out through a tube from the bladder (the urethra) from time to time when we go to the toilet.
Symptoms of a urine infection in children
It can be difficult to tell if a child has a urine infection. If they are very young they may not be able to let you know where the problem is. If they are still wearing nappies, you may not notice them passing urine more often.
Young children, toddlers and babies can have various symptoms which may include one or more of:
Being sick (vomiting) and/or diarrhoea.
Drowsiness.
Crying, going off feeds and generally seeming unwell.
Appearing to be in pain.
Blood in the urine (uncommon).
Cloudy or smelly urine.
Older children may say that they have pain when they pass urine, and pass urine frequently. If a kidney becomes infected they may also have shivers and complain of tummy (abdominal) pain, back pain, or a pain in a side of the abdomen. Bedwetting in a previously dry child is sometimes due to a children's urine infection. Just being generally unwell may be due to a urine infection.
Note: a urine infection should be suspected in any child who is unwell or has a fever with no other clear cause. This is why a urine test is commonly done when a child is unwell. It is important to diagnose and treat a urine infection in children promptly.
How is a urine infection in children confirmed?
A sample of urine is needed to confirm the diagnosis. Urine normally has no germs (bacteria) present, or only very few. A urine infection in children can be confirmed by urine tests which detect bacteria and/or the effects of infection in the urine.
Ideally, the sample of urine should not come into contact with skin or other materials which may contaminate it with other bacteria. Adults and older children can do this by a midstream collection of urine. This is not easy to do in young children and babies. The following are ways to obtain a sample of urine that is not contaminated:
Young children - the usual way is to catch some urine in the specimen bottle whilst they are passing urine. Just be ready with the open bottle as the child passes urine. (Be careful not to touch the open rim of the bottle with your fingers, as this may contaminate the specimen with bacteria from your fingers.)
Babies - one method is to place a specially designed absorbent pad in a nappy (supplied by a doctor). Urine is sucked into a syringe from the wet pad. Another method is to use a plastic bag that sticks on to the skin and collects urine. If no pad or plastic bag is available, the following might work. Take the nappy off about one hour after a feed. Gentle wiping of the skin over the pubic area, using gauze soaked in cold water, helps trigger peeing.
If you collect a sample at home, take it to the doctor or clinic as soon as possible after collection. If there is a delay, store the urine sample in the fridge.
If you are unable to obtain a sample by the methods above, there are other ways to obtain one. These ways are a little more uncomfortable and are usually done in hospital. A doctor could put a thin, flexible, hollow tube called a catheter into the bladder to get the sample. The tube is then taken out straightaway. Alternatively a doctor can also use a sterile needle to take a sample directly from the bladder, by going through the skin just above the pubic bone. A local anaesthetic is used to avoid hurting the child.
Treatment of a urine infection in children
A course of an antibiotic medicine will usually clear the infection within a few days. Depending on where the infection is and how severe it is, the antibiotics may be a three-day course up to a ten-day course.
Sometimes, for very young babies or for severe infections in hospital, antibiotics are given directly into a vein through a drip.
Give lots to drink to prevent a lack of fluid in the body (dehydration). Also, give paracetamol if needed to ease any pains and high temperature (fever).
How common is urine infection in children?
Around 1 in 30 boys and 1 in 10 girls have at least one urine infection by the time they are 16 years old.
Some terms used by doctors include:
Urinary tract infection (UTI) - which means a urine infection somewhere in the urinary tract.
Cystitis - which means infection or inflammation in the bladder.
Lower UTI - which means the infection is confined to the bladder and urethra. This is much the same as cystitis.
Upper UTI - the infection affects a kidney and/or a tube called a ureter.
Pyelonephritis - a term that means infection of a kidney.
Loin pain - which is a pain in one side of the back, often coming from a kidney.
Does anything increase the risk of developing a urine infection in children?
In most cases
No. In most urine infections in children, there is no underlying problem to account for it.
In some cases
Retaining some urine in the urinary tract may play a part. When we pass urine, the bladder should empty completely. This helps to flush out any germs (bacteria) that may have got into the bladder since the last toilet trip. However, some abnormalities or problems that affect the urinary tract can make some urine stay (be retained) in the bladder, kidney or urine tubes. This may allow any bacteria to multiply, as urine is a good food for some bacteria. This increases the chance of developing a urine infection in children. The following are the most common causes of retaining urine.
Constipation - if large hard stools (faeces) collect in the back passage (anus) they can press on the bladder. The bladder may then not empty fully when the child passes urine. Treating severe constipation sometimes prevents recurring urine infections in children.
Dysfunctional elimination syndrome - this is a condition where a child repeatedly holds on to urine and/or stools. That is, they regularly do not fully empty their bladder or bowel when they go to the toilet. There is no physical cause for this (that is, no abnormality in the urinary tract or rectum). The reason why this occurs is often unclear. Stress or emotional problems may be the underlying cause.
An abnormality of the urinary tract - structural abnormalities can cause retention of urine. The most common condition is called vesicoureteric reflux. This is a structural problem at the junction where the ureter tube enters the bladder. In this condition, urine is passed back (refluxes) up the ureter from the bladder from time to time. This should not happen. The urine should only flow downwards out of the bladder when going to the toilet.
This condition makes urine infections in children more likely. Infected urine that refluxes from the bladder back up to the kidneys may also cause kidney infection, scarring and damage. In some cases this leads to severe kidney damage if urine infections recur frequently. Other rare problems that may be found include kidney stones, or rare abnormalities of parts of the urinary tract.
Nerve (neurological) or spinal cord disorders - anything that affects the bladder emptying or sensation. These are rare in children.
Other conditions
Other conditions which increase the risk of a urine infection include having diabetes and having a poorly functioning immune system. For example, children having chemotherapy may have a less effective immune system.
What is the outlook (prognosis)?
In most cases, this is excellent. Once a child's urine infection is diagnosed and treated, the infection usually clears away and the child recovers fully. In many cases, a urine infection is a one-off event. However, some children have more than one urine infection and some develop several throughout their childhood (recurring UTIs).
In some cases, urine infections in children can be severe, particularly if a kidney becomes badly infected. This can sometimes be serious, even life-threatening in a minority of cases if treatment is delayed. A bad infection, or repeated infections, of a kidney may also do some permanent damage to the kidney. This could lead to kidney problems or high blood pressure later in life.
When are further tests advised?
Urine infection in children is common. In most cases, a child with a urine infection will make a full recovery.
Tests are advised in some cases to check on the kidneys and/or bladder. Your doctor will advise if your child needs further tests. It depends on factors such as the child's age, the severity of the infection and whether it has happened before. For example:
Children over the age of 6 months who have a one-off urine infection which promptly clears with treatment do not usually need any further tests.
Children with a severe infection, or with an infection with unusual features, may need tests.
Children who have two or more infections of any severity may need tests.
The tests that are advised may vary depending on local policies and the child's age. There are various tests (scans, etc) which may be used. These are to check on the structure and function of the urinary tract (the kidneys, the bladder and the tubes which carry urine).
The results of the tests are normal in most cases. However, in some cases, an abnormality such as vesicoureteric reflux may be detected (described above). Depending on whether an abnormality is detected, and how severe it is, a kidney specialist may advise a regular daily low dose of an antibiotic medicine. This treatment is advised in some cases to prevent further urine infections, with the aim of preventing damage to the kidneys.
Note: the general rules as to which children should have further tests following a urine infection have been laid out for England and Wales in guidelines from the National Institute for Health and Care Excellence (NICE). The guidance may differ in other countries. See the link to the NICE guideline in the Further Reading section below.
General tips following a urine infection in a child
To help to prevent a further infection in the future:
Try not to let your child become constipated. A good diet will help here. Ask your doctor for advice on this if you are not sure what foods are best to prevent constipation.
Make sure your child has plenty to drink each day.
Make sure your child is clean after going to the toilet, and teach them how to do this when they are old enough to go to the toilet alone.
Make sure your child can go to the toilet promptly when they need to; encourage them to do so. You may need to make a nursery/school teacher aware that your child has had a urine infection.
Also, consult a doctor promptly if you suspect your child has another urine infection. If this is confirmed, remind your doctor that your child has had a previous urine infection. Further tests may be advised.
Patient picks for Infections

Children's health
Coughs and colds in children
Coughs and colds are usually caused by infection with a germ called a virus. They normally clear away on their own. Antibiotic medicines don't help, and can cause harms, such as diarrhoea and vomiting. Paracetamol or ibuprofen may ease some of the symptoms. Make sure the child has enough to drink.
by Dr Doug McKechnie, MRCGP

Children's health
School exclusion for infections
This leaflet provides brief information about common childhood infections and whether or not children should go to school, nursery or other childcare.
by Dr Colin Tidy, MRCGP
Frequently asked questions
What is the difference between an upper and a lower urine infection?
A lower urine infection, also known as cystitis, means the infection is limited to the bladder and the urethra (the tube carrying urine out of the body). An upper urine infection, on the other hand, means the infection has travelled higher up to affect a kidney and/or the ureters (the tubes connecting the kidneys to the bladder). When a kidney is infected, it's called pyelonephritis.
If my child has had one urine infection, are they more likely to get another?
While many children experience a urine infection as a one-off event and recover fully, some children do have more than one infection. Recurring infections, particularly if they affect the kidneys, can sometimes lead to kidney damage or high blood pressure later in life. If your child has had a previous urine infection and you suspect another, it's important to tell your doctor as further tests or preventative measures might be considered.
Why do girls get urine infections more often than boys?
Around 1 in 10 girls will have at least one urine infection by the age of 16, compared to about 1 in 30 boys. The article does not directly explain why girls are more commonly affected, but it is a recognised pattern that often relates to anatomical differences in the urinary tract.
Can food or diet help prevent urine infections in children?
A good diet can help prevent constipation, which in turn can reduce the risk of urine infections. If severe constipation is treated, it can sometimes prevent recurring infections. It's recommended to ask your doctor for advice on the best foods to prevent constipation if you are unsure.
What should I do if my child needs to go to the toilet urgently at nursery or school, especially after having a urine infection?
It's important to make sure your child can go to the toilet promptly when they need to and encourage them to do so. You may need to inform their nursery or school teacher that your child has had a urine infection so they are aware and can accommodate your child’s needs.
Are there any specific cleaning techniques after using the toilet that can help prevent urine infections?
Yes, it’s important to make sure your child is clean after going to the toilet. As they get older, you should teach them how to clean themselves properly when they are able to go to the toilet alone.
Further reading and references
- Williams G, Craig JC; Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev. 2019 Apr 1;4:CD001534. doi: 10.1002/14651858.CD001534.pub4.
- Urinary tract infection in under 16s: diagnosis and management; NICE guideline (July 2022)
- Urinary tract infection - children; NICE CKS, April 2024 (UK access only)
- Leung AKC, Wong AHC, Leung AAM, et al; Urinary Tract Infection in Children. Recent Pat Inflamm Allergy Drug Discov. 2019;13(1):2-18. doi: 10.2174/1872213X13666181228154940.
- 't Hoen LA, Bogaert G, Radmayr C, et al; Update of the EAU/ESPU guidelines on urinary tract infections in children. J Pediatr Urol. 2021 Apr;17(2):200-207. doi: 10.1016/j.jpurol.2021.01.037. Epub 2021 Feb 2.
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Krishna Vakharia, MRCGP
Chief Medical Officer for Health, Optum UK
MBChB, MRCGP(2013), BMedSci (hons), DFSRH, DRCOG, PGDipDerm (Distn)
Dr Krishna Vakharia is an NHS GP. She is also a regular examiner for the postgraduate Diploma in Practical Dermatology at Cardiff University as well as being the Chief Medical Officer for health at Optum UK.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 25 Aug 2027
26 Aug 2022 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in children's health
- Anxiety in children
- Baby-led weaning
- Bedwetting
- Blocked nose in babies
- Breastfeeding your baby
- Breathing difficulties in children
- Children's cancers
- Cot death
- Eczema in children
- Hirschsprung's disease
- Intussusception and volvulus in children
- Knock knees
- Nausea and vomiting
- Rhabdomyosarcoma
- Seborrhoeic dermatitis in babies
- Spina bifida
- Surviving adolescence
- Tear duct blockage in babies
- Wilms' tumour