Peripheral arterial disease
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 21 Aug 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
Peripheral arterial disease, also called peripheral vascular disease, is a narrowing of the blood vessels (arteries). In addition to also being known as peripheral vascular disease (PVD), it is also sometimes called 'hardening' of the arteries of the legs.
At a glance
Peripheral arterial disease (PAD) is the narrowing of blood vessels, mainly in the legs.
The main symptom is leg pain when walking, which eases with rest.
Poor hair growth, cool feet, and weak pulses can also be signs.
A doctor can diagnose PAD by comparing blood pressure in your ankle and arm.
Lifestyle changes like stopping smoking and regular exercise are important treatments.
Medicines may be prescribed to reduce clot formation and lower cholesterol.
Surgery is rarely needed but may involve angioplasty, bypass, or, in severe cases, amputation.
In this article:
Video picks for Arteries
Continue reading below
What is peripheral arterial disease?
Peripheral arterial disease (PAD) is narrowing of one or more blood vessels (arteries). It mainly affects arteries that take blood to your legs. (Arteries to the arms are rarely affected and are not dealt with further in this leaflet.) The narrowing of blood vessels (arteries) is caused by atheroma. The main symptom is pain in one or both legs when you walk.
In the UK, around 1 in 5 men and 1 in 8 women aged 50-75 years have PAD. It becomes more common with increasing age.
Symptoms of peripheral arterial disease
Back to contentsThe typical symptom of peripheral arterial disease is pain which develops in one or both calves when you walk or exercise and is relieved when you rest for a few minutes. This pain varies between cases and you may feel aching, cramping or tiredness in your legs.
This is called intermittent claudication. It is due to narrowing of one (or more) of the blood vessels (arteries) in your leg. The most common artery affected is the femoral artery.
When you walk, your calf muscles need an extra blood and oxygen supply. The narrowed artery cannot deliver the extra blood and so pain occurs from the oxygen-starved muscles. The pain comes on more rapidly when you walk up a hill or stairs than when on the flat.
If an artery higher upstream is narrowed, such as the iliac artery or aorta, then you may develop pain in your thighs or buttocks when you walk.
If the blood supply to the legs becomes worse, the following may be found by a doctor who examines you:
Poor hair growth below your knee and poor toenail growth.
Cool feet.
Weak or no pulses in the arteries of your feet.
Severe cases of peripheral arterial disease
If the blood supply is very much reduced then you may develop pain even at rest, particularly at night when the legs are raised in bed. Typically, rest pain first develops in the toes and feet rather than in the calves.
Sores (ulcers) may develop on the skin of your feet or lower leg if the blood supply to the skin is poor. In a small number of cases, tissue death (gangrene) of a foot may result. However, this is usually preventable (see below).
Continue reading below
Peripheral arterial disease tests
Back to contentsThe diagnosis is usually made by the typical symptoms. A simple test that your doctor or nurse may do is to check the blood pressure in your ankle and compare this to the blood pressure in your arm. This is called the ankle brachial pressure index (ABPI).
If the blood pressure in your ankle is much different to that in your arm then this usually means that one or more blood vessels (arteries) going to your leg, or in your leg, are narrowed. However, the ABPI can be normal in some cases. Although this test can help your doctor find out if PAD is affecting your legs, it will not identify which blood vessels are blocked.
More sophisticated tests are not needed in most cases. They may be done if the diagnosis is in doubt, or if surgery is being considered (which is only in the minority of cases). For example, a computerised tomography (CT) scan, a magnetic resonance imaging (MRI) scan or an ultrasound scan of the arteries can build up a map of your arteries and show where they are narrowed.
What is the outlook (prognosis) for peripheral arterial disease?
Back to contentsStudies that have followed up people with PAD have shown that:
Symptoms remain stable or improve in about 15 out of 20 cases.
Symptoms gradually become worse in about 4 out of 20 cases.
Symptoms become severe in about 1 out of 20 cases.
So, in most cases, the outlook for the legs is quite good.
However, if you have PAD, it means that you have an increased risk of developing fatty patches (atheroma) in other blood vessels (arteries). You have around a 6-7 higher-than-average risk of developing heart disease (such as angina or a heart attack) or of having a stroke.
The main concern for most people with PAD is this increased risk of having a heart attack or stroke.
Note: your chance of developing severe PAD (and heart disease or a stroke) is much reduced by the self-help measures and treatments described below.
Continue reading below
What self-help measures can I do?
Back to contentsPeripheral arterial disease treatment
Back to contentsThe self-help measures above are the most important part of treatment. In addition, medication is often advised. Surgery is only needed in a small number of cases.
Medicines
A medicine called clopidogrel is usually advised. This does not help with symptoms of PAD but helps to prevent blood clots (thromboses) forming in blood vessels (arteries). It does this by reducing the stickiness of platelets in the bloodstream. If you cannot take clopidogrel then alternative antiplatelet medicines such as low-dose aspirin may be advised.
A statin medicine is usually advised to lower your cholesterol level. This helps to prevent a build-up of fatty patches (atheroma).
If you have diabetes then good control of your blood sugar (glucose) level will help to prevent PAD from worsening.
If you have high blood pressure (hypertension) then you will normally be advised to take medication to lower it.
Other medicines are sometimes used to try to open up the arteries - for example, cilostazol and naftidrofuryl. One may be given and may help. However, they do not work in all cases. Therefore, there is no point in continuing with these medicines if you do not notice an improvement in symptoms within a few weeks.
Surgery
Most people with PAD do not need surgery. Your GP may refer you to a surgeon if symptoms of PAD become severe, particularly if you have pain when you are resting. Surgery is considered a last resort. There are three main types of operation for PAD:
Angioplasty - in this procedure, a tiny balloon is inserted into the artery and blown up at the section that is narrowed. This widens the affected segment of artery. This is only suitable if a short segment of artery is narrowed.
Bypass surgery - in this procedure, a flexible pipe (graft) is connected to the artery above and below a narrowed section. The blood is then diverted around the narrowed section.
Surgical removal (amputation) of a foot or lower leg - this is needed in an extremely small number of cases. It is only offered when all other options have been considered. It is needed when severe PAD develops and a foot has tissue death (becomes gangrenous) due to a very poor blood supply.
Patient picks for Arteries
Heart health and blood vessels
Giant Cell Arteritis
Giant cell arteritis is also known as temporal arteritis. The typical symptoms of giant cell arteritis (temporal arteritis) are headache, tenderness over one or both sides of the forehead, and feeling generally unwell. Other symptoms that may occur include pain in your jaw muscles when chewing, and visual loss. Seek medical attention immediately if you suspect that you have giant cell arteritis. People with giant cell arteritis need urgent treatment with steroids. Prompt treatment aims to prevent serious complications such as severe sight impairment which can occur soon after the disease starts.
by Dr Philippa Vincent, MRCGP
Heart health and blood vessels
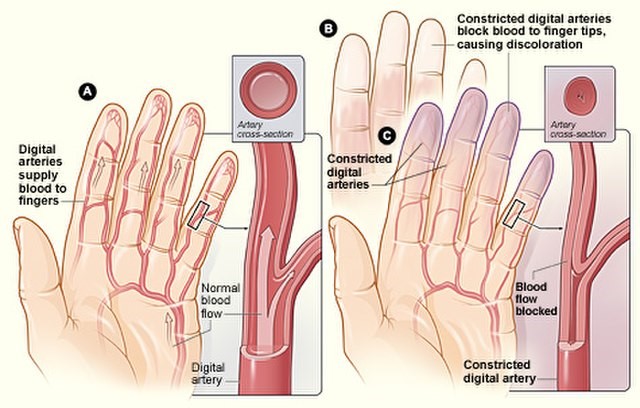
Raynaud's phenomenon
Raynaud's phenomenon (often just called Raynaud's), is a condition where the small blood vessels of the fingers become narrow (constrict). This happens most often when they are in a cool environment. Blood vessels to other extremities such as the toes, ears and nose may also be affected. It is named after Dr Maurice Raynaud, the man who first described it in 1862.
by Dr Hayley Willacy, FRCGP
Frequently asked questions
What specifically causes the pain in my legs when I walk with PAD?
The pain you feel when walking is due to your calf muscles not getting enough blood and oxygen. When you exercise, your muscles need more blood, but the narrowed arteries in your legs can't deliver it. This lack of oxygen to the muscles causes the pain, which varies between aching, cramping, or tiredness.
Can I prevent PAD from getting worse using self-help measures?
Yes, self-help measures can significantly reduce your chance of severe PAD and related issues like heart disease or stroke. These include stopping smoking, exercising regularly, losing weight if you are overweight, eating a healthy diet, and taking care of your feet.
How important is the ABPI test for diagnosing PAD?
The Ankle Brachial Pressure Index (ABPI) test is a simple and common way to diagnose PAD. It compares blood pressure in your ankle to your arm. If there's a significant difference, it suggests narrowed arteries in your leg. While useful, it might be normal in some cases and doesn't pinpoint which specific blood vessels are blocked.
Why would a doctor examine my feet and hair growth if I have leg pain?
If the blood supply to your legs is significantly reduced, a doctor might look for signs like poor hair growth below your knees, poor toenail growth, cool feet, or weak/absent pulses in your feet. These physical signs can indicate the severity of the blood circulation problem caused by PAD.
Are there medicines that can open up the narrowed arteries in my legs?
Some medicines like cilostazol and naftidrofuryl are occasionally used to try and open up arteries. They may help in some cases, but they don't work for everyone. If you don't notice an improvement in your symptoms within a few weeks, there's no benefit in continuing them.
If I have PAD, am I at higher risk of other health problems?
Yes, if you have PAD, it means you have an increased risk of developing fatty patches in other arteries throughout your body. You have a significantly higher risk (around 6-7 times the average) of developing heart disease, such as angina or a heart attack, or of having a stroke.
Further reading and references
- Clopidogrel and modified-release dipyridamole for the prevention of occlusive vascular events; NICE Technology appraisal guidance, December 2010
- Peripheral arterial disease - cilostazol, naftidrofyryl oxalate, pentoxifylline and inositol nicotinate; NICE Technology Appraisal Guidance, May 2011
- Lower limb peripheral arterial disease; NICE Clinical Guideline (August 2012, updated December 2020)
- Aboyans V, Ricco JB, Bartelink MEL, et al; 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2017 Aug 26. doi: 10.1093/eurheartj/ehx095.
- Peripheral Arterial Disease; NICE CKS, March 2024 (UK access only)
- Zemaitis MR, Boll JM, Dreyer MA; Peripheral Arterial Disease.
Continue reading below
About the authorView full bio

Dr Hayley Willacy, FRCGP
General Practitioner, Medical Author
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
Dr Hayley Willacy was an NHS GP working in northwest England, who retired from clinical practice in 2022 after 30 years.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 19 Aug 2028
21 Aug 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.