Coronary artery spasm
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Hayley Willacy, FRCGP Last updated 17 Nov 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
In this series:AnginaMicrovascular angina
Coronary artery spasm is a temporary, sudden narrowing of one or more of the coronary arteries.
In this article:
Video picks for Arteries
Continue reading below
What is a coronary artery spasm?
The spasm slows or stops blood flowing through the artery and so reduces the blood supply to the heart muscle. Coronary artery spasm is sometimes called variant angina or Prinzmetal's angina. Angina is a medical term for chest pain.
Symptoms of a coronary artery spasm
Back to contentsCoronary artery spasm may occur without any symptoms. The most common symptom is heart chest pain (angina). If the coronary artery spasm is severe and lasts long enough then it may cause a heart attack (myocardial infarction).
Chest pain (angina)
With angina, the pain is usually described as:
Severe pain that can be felt under the breast bone (sternum) or on the left side of the chest.
A feeling of crushing, pressure, squeezing or tightness.
A pain that spreads to the neck, jaw, shoulder or arm. It may feel like it's in the back.
The chest pain caused by coronary artery spasm often occurs at rest and commonly doesn't occur during exercise. This is very different from angina due to fatty patches or plaques (atheroma), when the pain is usually triggered by exercise and goes away when you rest.
The chest pain may occur at the same time each day and most often occurs during the night and early morning. The pain can be very variable but usually lasts between 5 and 30 minutes. It can occasionally spread to the back. The pain does not improve with change of position, unlike pericarditis, which is sometimes relieved by leaning forward.
Coronary artery spasm may also cause shortness of breath. A severe episode of coronary artery spasm may cause a loss of consciousness.
Continue reading below
Causes of a coronary artery spasm
Back to contentsCoronary artery spasm often occurs in coronary arteries that have not already become blocked with fatty patches or plaques (atheroma). However, coronary artery spasm can also occur in coronary arteries that are already partially blocked with atheroma.
Coronary artery spasm may occur without any obvious cause. At other times the spasm may be triggered by various factors such as:
Emotional stress.
Alcohol.
Exposure to cold.
Stimulant drugs (such as amphetamines and cocaine).
What else could it be?
Back to contentsCoronary artery spasm is sometimes mistaken for other heart-related (cardiac) causes of chest pain such as pericarditis, a heart attack and cardiomyopathy. Non-cardiac causes of chest or upper tummy pain may need to be ruled out such as gallbladder disease and stomach ulcers.
Continue reading below
How common is a coronary artery spasm?
Back to contentsAbout 1 person in every 50 with angina has coronary artery spasm. Coronary artery spasm is more common in males and those aged between 40 and 70 years.
Coronary artery spasm is more common in people who:
Smoke.
Have high blood pressure.
Have high blood cholesterol level.
However, coronary artery spasm may occur without any risk factors for heart disease such as smoking, diabetes, high blood pressure and high cholesterol.
Diagnosing a coronary artery spasm
Back to contentsIf you are thought to have heart chest pain (angina), you will usually be referred to see a specialist for investigations.
The initial investigations will include:
A 'heart tracing' (electrocardiogram, or ECG).
Other investigations may also be used, including:
The coronary angiogram may be normal if there is no blockage of the coronary arteries caused by fatty patches or plaques (atheroma). However, coronary artery spasm can be triggered by injecting a chemical into one of your veins. This is called a provocation test.
The chemical is otherwise safe and the coronary angiogram may then show temporary narrowing of the coronary arteries in people with coronary artery spasm.
Coronary artery spasm treatment
Back to contentsThe aim of treatment is to control chest pain and to prevent a heart attack (myocardial infarction). The most important aspects of treatment are to avoid any known triggers for coronary artery spasm and to reduce the risk of heart disease. Reducing the risk of heart disease includes:
Lifestyle advice to stop smoking, eat a healthy diet, have regular exercise and reduce body weight if overweight.
Medicines may be needed, such as to control high blood pressure or a high cholesterol level.
See the separate leaflet called Cardiovascular disease (Atheroma).
Glyceryl trinitrate (GTN) can be used to relieve an episode of chest pain. Your healthcare provider may prescribe other medicines to prevent chest pain. You may also need a type of medicine called a calcium-channel blocker or a long-acting nitrate. Beta-blockers should be avoided because they may make this condition worse.
You will need to be referred to a heart specialist for further investigations and treatment. Further treatments may include coronary angioplasty if you also have coronary artery blockage caused by fatty patches or plaques (atheroma).
An implantable cardioverter defibrillator may be needed if you are at risk of life-threatening abnormal heart rhythms caused by coronary artery spasm. See the separate leaflet called Abnormal heart rhythms (Arrhythmias) for more details.
Complications of a coronary artery spasm
Back to contentsCoronary artery spasm may cause an abnormal heart rhythm (arrhythmia), which may be life-threatening. Severe and prolonged coronary artery spasm may cause a heart attack (myocardial infarction).
What is the outcome?
Back to contentsCoronary artery spasm is a long-term condition. However, treatment most often helps to control symptoms. The outcome (prognosis) for people with coronary artery spasm is generally good if they follow treatment recommendations and avoid certain triggers.
The outcome is not as good in people who also have blockage of the coronary arteries caused by fatty patches or plaques (atheroma).
Patient picks for Arteries
Heart health and blood vessels
Giant Cell Arteritis
Giant cell arteritis is also known as temporal arteritis. The typical symptoms of giant cell arteritis (temporal arteritis) are headache, tenderness over one or both sides of the forehead, and feeling generally unwell. Other symptoms that may occur include pain in your jaw muscles when chewing, and visual loss. Seek medical attention immediately if you suspect that you have giant cell arteritis. People with giant cell arteritis need urgent treatment with steroids. Prompt treatment aims to prevent serious complications such as severe sight impairment which can occur soon after the disease starts.
by Dr Philippa Vincent, MRCGP
Heart health and blood vessels
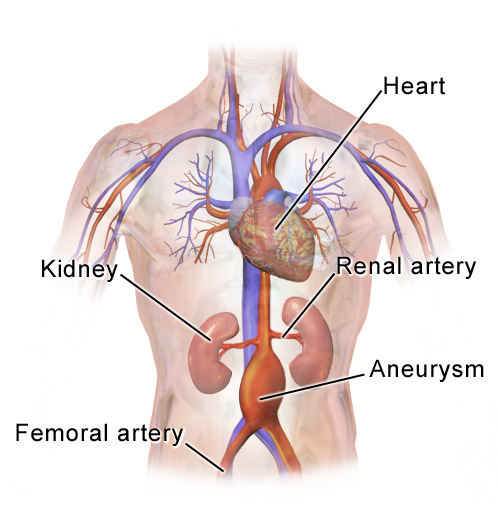
Abdominal aortic aneurysm
The aorta is the main blood vessel in the abdomen, running down from your heart. It is normally about the diameter of a garden hose. In older people, particularly those who smoke, part of it can enlarge and balloon up. This is called an abdominal aortic aneurysm (often abbreviated to AAA, pronounced 'triple-A'). This doesn't cause any symptoms and the person is usually unaware they have it, until it leaks or bursts. The medical term for this is rupture. If the aneurysm ruptures, it can be fatal. In the UK there is a screening programme for men over the age of 65, to see if they have a triple-A. An operation to repair the aneurysm may be advised if it is larger than 5.5 cm, as above this size the risk of rupture increases significantly.
by Dr Doug McKechnie, MRCGP
Further reading and references
- Swarup S, Patibandla S, Grossman SA; Coronary Artery Vasospasm.
- Matta A, Bouisset F, Lhermusier T, et al; Coronary Artery Spasm: New Insights. J Interv Cardiol. 2020 May 14;2020:5894586. doi: 10.1155/2020/5894586. eCollection 2020.
- Teragawa H, Oshita C, Ueda T; Coronary spasm: It's common, but it's still unsolved. World J Cardiol. 2018 Nov 26;10(11):201-209. doi: 10.4330/wjc.v10.i11.201.
- Assessing fitness to drive: guide for medical professionals; Driver and Vehicle Licensing Agency
Continue reading below
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 16 Nov 2027
17 Nov 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.