Stroke
Peer reviewed by Dr Doug McKechnie, MRCGPLast updated by Dr Colin Tidy, MRCGPLast updated 10 Sept 2024
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In this series:Transient ischaemic attack
A stroke causes damage to the brain. A common cause of stroke is a blood clot that forms in a brain blood vessel (artery). Immediate treatment may include a clot-busting medicine to dissolve the blood clot. Other treatments include medication to reduce risk factors for further strokes. Rehabilitation is a major part of treatment.
Having a stroke is a medical emergency. Disability following a stroke depends on factors such as the part of the brain affected, how quickly treatment was given and the extent of the damage to the brain. Call for an ambulance immediately if you suspect someone is having a stroke. Common symptoms are listed below.
At a glance
A stroke means the blood supply to part of the brain is suddenly cut off.
The FAST test (Face, Arms, Speech, Time) helps recognise a stroke.
Call 999 immediately if you suspect a stroke, as it is a medical emergency.
Symptoms vary depending on the part of the brain affected.
A transient ischaemic attack (TIA) has similar symptoms but they last less than 24 hours.
Early treatment can include clot-busting medicines or surgical removal of a clot.
Rehabilitation is vital after a stroke to maximise recovery and quality of life.
A quick guide for the general public to remember
Both a stroke and a transient ischaemic attack (TIA) are medical emergencies and need immediate medical attention. As a way of helping the general public to become more aware of the symptoms of a stroke or TIA, a simple symptom checklist is to think of the word FAST. That is:
Facial weakness. Can the person smile? Has their mouth or eye drooped?
Arm weakness. Can the person raise both arms?
Speech disturbance. Can the person speak clearly? Can they understand what you say?
Time to call 999/112/911.
If any of these symptoms suddenly develop then the person needs to see a doctor urgently. So call an ambulance FAST. The FAST checklist does not cover every possible symptom of stroke or TIA. However, it is easy to remember and it is estimated that about 8 or 9 in 10 people with a stroke or TIA will have one or more FAST symptoms. See below for other symptoms that indicate the possibility of a stroke.
Stroke symptoms
The functions of the different parts of the body are controlled by different parts of the brain. So, the symptoms vary depending on which part of the brain is affected and on the size of the damaged area. Symptoms develop suddenly and usually include one or more of the following:
Weakness of an arm, leg, or both. This may range from total paralysis of one side of the body to mild clumsiness of one hand.
Weakness and twisting of one side of the face. This may cause you to drool saliva, or cause slurred speech.
Problems with balance, co-ordination, vision, speech, communication or swallowing.
Dizziness or unsteadiness.
Numbness in a part of the body.
Confusion.
Loss of consciousness (occurs in severe cases).
What causes a stroke?
What is a stroke?
A stroke means that the blood supply to a part of the brain is suddenly cut off. The brain cells need a constant supply of oxygen from the blood. Soon after the blood supply is cut off, the cells in the affected area of brain become damaged or die. A stroke is sometimes called a brain attack.
The blood supply to the brain comes mainly from four blood vessels (arteries) - the right and left carotid arteries and the right and left vertebrobasilar arteries (see diagram below). These branch into many smaller arteries which supply blood to all areas of the brain. The area of brain affected and the extent of the damage depend on which blood vessel is affected.
For example, if you lose the blood supply from a main carotid artery then a large area of your brain is affected, which can cause severe symptoms or death. In contrast, if a small branch artery is affected then only a small area of brain is damaged which may cause relatively minor symptoms.
Stroke types
There are two main stroke types - ischaemic and haemorrhagic.
Stroke
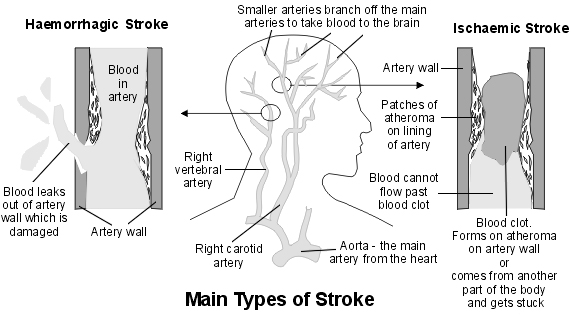
Ischaemic stroke - caused by a blood clot
Ischaemic means a reduced blood and oxygen supply to a part of the body. It is usually caused by blood clot in an artery, which blocks the flow of blood. This occurs in about 8 in 10 cases.
The blood clot often forms within the artery itself. This commonly occurs over a patch of fatty material called atheroma. Atheroma is often called furring or hardening of the arteries. Small patches of atheroma form on the inside of arteries in most older people. If a patch of atheroma becomes thick, it can trigger the blood to clot.
In some cases, the blood clot forms in another part of the body and then travels in the bloodstream - this is called an embolus. The most common example is a blood clot which forms in a heart chamber as a result of abnormal turbulent blood flow. This may occur in a condition called atrial fibrillation. See the separate leaflet called Atrial fibrillation for more details. The blood clot is then carried in the bloodstream until it gets stuck in an artery in the brain.
There are other rare causes of ischaemic stroke.
Haemorrhagic stroke - caused by bleeding
About 2-3 out of 20 strokes are caused by a bleed into the brain. A damaged or weakened artery may burst and bleed:
An intracerebral haemorrhage occurs when the blood vessel bursts inside the brain. The blood then spills into the nearby brain tissue. This can cause the affected brain cells to lose their oxygen supply. They become damaged or die. This happens in about 1 in 10 strokes.
A subarachnoid haemorrhage occurs when a blood vessel bursts in the subarachnoid space. This is the narrow space between the brain and the skull. This space is normally filled with a fluid called the cerebrospinal fluid. About 1 stroke in 20 is due to a subarachnoid haemorrhage.
Rarer causes
Rarer causes of stroke include cerebral venous thrombosis and carotid artery dissection.
Who is affected by stroke?
Each year around 120,000 people in the UK have a first stroke and about 30,000 have a recurrent stroke. Stroke is the largest cause of disability in the UK and the third most common cause of death (after heart disease and cancer). Most cases occur in people aged over 65 years. Each year about 1 in 100 people over the age of 75 years will have a stroke. But a stroke can occur at any age - even in babies. About one million people in the UK are living with the effects of stroke. Half of these people depend on others for help with everyday activities.
What is a transient ischaemic attack?
A transient ischaemic attack (TIA) causes symptoms similar to a stroke but the symptoms last for less than 24 hours. It is due to a temporary lack of blood to a part of the brain. In most cases, a TIA is caused by a tiny blood clot that becomes stuck in a small blood vessel (artery) in the brain. This blocks the blood flow and a part of the brain is starved of oxygen. The affected part of the brain is without oxygen for just a few minutes and soon recovers. This is because the blood clot either breaks up quickly or nearby blood vessels are able to compensate.
Unlike a stroke, the symptoms of a TIA soon go. However, you should see a doctor urgently if you have a TIA, as you are at increased risk of having a full stroke. People who have a TIA should be referred immediately for specialist assessment and seen within 24 hours of their symptoms starting. See the separate leaflet called Transient ischaemic attack for more details.
After effects of a stroke
The type and extent of disability caused by a stroke can vary greatly. It depends on the extent of the damage to the brain.
Brain cross-section
A large stroke can cause death. A small stroke may cause minor problems, which may go completely over time. In many cases the effects are somewhere in between these two extremes.
The signs of a stroke that may occur include one or more of the following:
Weakness of one side of the body. This may cause problems with walking if a leg is affected or problems using an arm or hand properly.
Problems with balance and co-ordination.
Swallowing problems are common. In some cases this can be dangerous, as food may go down the windpipe rather than down the gullet when you eat. Because of this, it is usual to do a swallow test on all people with a stroke before they are allowed to eat or drink. This is to make sure that swallowing is safe. If there is severe difficulty with swallowing then you may need to have food and drinks passed into your stomach via a tube.
Speech and communication difficulties. This may range from a difficulty in finding the correct words to say in the middle of a sentence to being completely unable to speak. Also, understanding speech, reading or writing may be affected.
Difficulty with vision. If a part of the brain that deals with vision is affected then problems may arise. For example, some people who have had a stroke have double vision. Some people lose half of their field of vision.
Difficulties with mental processes. For example, difficulty in learning, concentrating, remembering, etc.
Inappropriate emotions. For example, following a stroke, some people cry or laugh at times for no apparent reason.
Tiredness.
The above are just some examples of what may occur following a stroke. Every stroke is different and the problems and difficulties have to be assessed for each affected person.
In the first few weeks after a stroke the swelling and inflammation around the brain damage settles down. Some symptoms may then improve. In time, sometimes other parts of the brain can compensate for the damaged part of the brain. With rehabilitation and appropriate therapy, there may be a gradual improvement.
Of those people who survive a stroke, about 3 in 10 are fully independent within three weeks. This rises to about 5 in 10 within six months. However, it is common for some degree of disability to remain. People who have a haemorrhagic stroke are more likely to have severe symptoms and greater long-term disability.
Are any tests needed?
A doctor can usually diagnose a stroke by the typical symptoms and signs which develop suddenly. Tests which are commonly done include:
A brain scan (CT scan or MRI scan). This can determine the type of stroke (ischaemic or haemorrhagic) and may detect rarer conditions which may have caused the stroke or which may mimic a stroke.
Blood tests to check on such things as blood sugar level and cholesterol level. High levels can increase the risk of a further stroke.
Chest X-ray and a heart tracing (electrocardiogram, or ECG) to check for heart or lung conditions which may be a cause of stroke (for example, atrial fibrillation).
Ultrasound scan of the carotid blood vessels (arteries) in the neck to check if there are large patches of atheroma in these arteries.
Stroke treatment
If you suspect that you (or a person you are with) are having a stroke then call for an ambulance immediately. You should be admitted to hospital.
Immediate care
Ideally, you will be assessed quickly by a doctor. Commonly, a scan of the brain is organised as soon as possible. The aim of the scan is to confirm the diagnosis and to tell whether the stroke is an ischaemic or haemorrhagic stroke. This is very important to know, as the initial treatment of the two is very different.
Thrombolysis (clot-busting)
If an ischaemic stroke is diagnosed and it has been less than four and half hours since symptoms started, you will usually be given a medicine (alteplase or tenecteplase), directly into a vein (as long as there is no medical reason why you should not have this). This is a clot-busting medicine which aims to dissolve the blood clot. The medical word for this is thrombolysis. If the blood clot that caused the stoke can be dissolved shortly after symptoms begin, it can improve the eventual outcome. This is because brain cells that would have died are able to survive.
Clot removal
Sometimes an ischaemic stroke affects the front part of the brain (called the proximal anterior circulation). If you have a severe stroke affecting this region and it has been less than six hours since symptoms started, you may be offered thrombectomy - a surgical procedure to remove the clot. This is given alongside thrombolysis (above). The sooner this treatment is given, the more successful it is likely to be. In some circumstances, clot removal may be offered if the stroke symptoms started 6-24 hours ago if you were well before the stroke. This will only be considered if the scans show there is a chance of the brain tissue affected recovering.
The operation can be done under local or general anaesthetic. A small tube called a catheter is usually passed up an artery, often from your groin, into the brain. A small device on the end of the catheter is used to lift out or suck out the clot.
Further early treatment
A plan for any other medical treatment for stroke should be devised and started as soon as possible. Treatments should be tailored to the particular need of the individual. The treatment plan can depend on factors such as the severity of the stroke, the effects it has, the cause of the stroke, and other diseases that may be present. Treatments that may be considered include the following:
Antiplatelet medication. Platelets are tiny particles in the blood which help blood to clot. Antiplatelet medication is usually advised if you have had an ischaemic stroke (due to a blood clot). Antiplatelet medication reduces the stickiness of platelets. This helps to prevent blood clots forming inside arteries, which helps to prevent a further stroke. Aspirin (low-dose) is the most commonly used antiplatelet medicine when the stroke has just happened. Another antiplatelet medicine called clopidogrel is usually given long-term after the initial treatment.
Blood pressure control. Raised blood pressure is a major risk factor for stroke. If you have a bleed into the brain, your medical team will consider medication to bring your blood pressure down rapidly to bring the upper (systolic) blood pressure level to 130-140 mm Hg and keep it below this level for at least seven days.
If you have had an ischaemic stroke, your blood pressure should be controlled in the longer term. However, in the short term, blood pressure-lowering medication is not usually recommended.
Early mobilisation. Your team will encourage you to sit out of bed, stand or walk as soon as you are able, to reduce the risk of complications such as a clot on the leg which can travel to the lungs. It can also help reduce your risk of long-term disability.
If you are unable to swallow, you will be given food and fluids via a tube that is passed into your stomach. As mentioned earlier, a swallowing test is usually done early after being admitted to hospital.
Medication may be advised to reduce any risk factors for having a further stroke (as discussed later in this leaflet). For example, medication to lower a raised sugar level or cholesterol level.
If you have atrial fibrillation, you have an increased risk of a blood clot forming in a heart chamber and travelling to the brain to cause a stroke. If you have atrial fibrillation (or certain other heart conditions), an anticoagulant medicine (such as warfarin, dabigatran, apixaban or rivaroxaban) may be prescribed. Anticoagulant medicines help to prevent blood clots forming.
If you have carotid stenosis then you have an increased risk of having a stroke. Carotid stenosis means a narrowing of one of your carotid arteries, due to atheroma. If the narrowing is severe, you may be advised to have surgery to strip out the atheroma. Your doctor will advise if this is an option.
If you have a bleeding (haemorrhagic) stroke and are already taking an anticoagulant medicine, treatment to reverse the effect of the anticoagulation is given.
If a subarachnoid haemorrhage is the cause of the stroke, an operation to fix the leaking blood vessel (artery) is sometimes an option.
Other operations are occasionally done. For example, sometimes surgery is considered to ease the pressure within the skull if the pressure becomes high following certain types of stroke.
As soon as possible after having a stroke you should be helped to sit up in bed and to get out of bed and move around if you are able to do so. This is to start the process of rehabilitation as soon as possible. Also, this reduces the risk of having a deep vein thrombosis (DVT) in a leg vein, which is a risk if you are inactive in bed for long periods.
Rehabilitation
The aim of rehabilitation is to maximise activity and quality of life following a stroke. Hospitals which deal with stroke patients have various specialists who help in rehabilitation. These include physiotherapists, occupational therapists, speech therapists, dieticians, psychologists, specialist nurses and doctors.
One or more of these may be required, depending on how the stroke has affected you. Good-quality rehabilitation is vital following a stroke and can make a big difference to your eventual outcome. See also the separate article called How to cope with isolation after a stroke.
How to prevent a stroke
As described above, a common reason why a blood clot forms is because it develops over a patch of atheroma on the lining of a blood vessel (artery). Certain risk factors increase the chance of atheroma forming - which increase your risk of having a stroke (and heart attack). You can reduce your chances of having a stroke (or a further stroke) if you reduce your risk factors. Briefly, risk factors that can be modified are:
Smoking. If you smoke, you should make every effort to stop. The chemicals in tobacco are carried in your bloodstream and can damage your arteries. If you smoke, stopping smoking can greatly cut your risk of having a stroke.
High blood pressure. Make sure your blood pressure is checked at least once a year. If it is high it can be treated. High blood pressure usually causes no symptoms but can be damaging to the arteries. If you have high blood pressure, treatment of the blood pressure is likely to have the greatest effect on reducing your risk of having a stroke.
If you are overweight, losing some weight is advised.
A high cholesterol level. This can be treated if it is high. See High cholesterol for more information.
Inactivity. If able, you should aim to do some moderate physical activity on most days of the week for at least 30 minutes. For example, brisk walking, swimming, cycling, dancing, gardening, etc.
Diet. You should aim to eat a healthy diet. See Healthy eating for more information.
Alcohol. Men and women should drink no more than 14 units of alcohol per week. These units should be spread out through the week and there should be at least two alcohol-free days each week. See Alcohol and sensible drinking - safe limits of alcohol.
Diabetes is a risk factor. If you have diabetes, treatment to keep your blood sugar as near normal as possible is important.
See the separate feature Your guide to stroke prevention for more details.
People with atrial fibrillation have an increased risk of having a stroke. This increased risk can also be reduced. See the separate leaflet called Atrial fibrillation and stroke prevention for more details.
Patient picks for Stroke
Frequently asked questions
How quickly do stroke symptoms appear?
Stroke symptoms develop suddenly. The functions of different parts of the body are controlled by different areas of the brain, so the specific symptoms depend on which part of the brain is affected and the size of the damaged area.
Can a stroke cause mental or emotional changes?
Yes, a stroke can lead to difficulties with mental processes, such as learning, concentrating, or remembering. It can also cause inappropriate emotions, where some people might cry or laugh at unexpected times without an apparent reason.
What is the difference between a stroke and a TIA?
Both a stroke and a transient ischaemic attack (TIA) are medical emergencies with similar symptoms. The key difference is that TIA symptoms last for less than 24 hours because the temporary lack of blood to the brain is resolved quickly, unlike a stroke where brain cells are damaged or die. Even though TIA symptoms go away, it's crucial to see a doctor urgently as it increases the risk of a full stroke.
Is it possible for a person to recover completely from a stroke?
While many people experience some degree of long-term disability, some individuals can achieve a good level of recovery. About 3 in 10 stroke survivors are fully independent within three weeks, increasing to about 5 in 10 within six months. The extent of recovery depends on the damage, early treatment, and effective rehabilitation.
What kind of medical professionals are involved in stroke rehabilitation?
Stroke rehabilitation involves a team of specialists to help maximise activity and quality of life. This team can include physiotherapists, occupational therapists, speech therapists, dieticians, psychologists, specialist nurses, and doctors, depending on the individual's needs and how the stroke has affected them.
Why is early mobilisation important after a stroke?
Early mobilisation, such as sitting out of bed, standing, or walking as soon as possible, is encouraged to reduce the risk of complications like deep vein thrombosis (DVT), which is a blood clot in the leg that can travel to the lungs. It also helps in starting the rehabilitation process quickly and can reduce the risk of long-term disability.
Are there any rare causes of stroke?
Yes, in addition to ischaemic (blood clot) and haemorrhagic (bleeding) strokes, there are rarer causes. These include cerebral venous thrombosis, which involves a blood clot in the brain's veins, and carotid artery dissection, where a tear in the wall of a carotid artery reduces blood flow to the brain.
Further reading and references
- Stroke and transient ischaemic attack in over 16s: diagnosis and initial management; NICE Guidance (May 2019 - last updated April 2022)
- Stroke and TIA; NICE CKS, December 2023 (UK access only)
- Stroke rehabilitation in adults; NICE guidance (October 2023)
- Alteplase for treating acute ischaemic stroke; NICE Technology appraisal guidance (TA264). September 2012.
- Tenecteplase for treating acute ischaemic stroke; NICE Technology appraisal guidance, July 2024
- State of the Nation - Stroke statistics; Stroke Association 2023
- Cardiovascular disease prevention; NICE Public Health Guideline (June 2010)
About the authorView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
About the reviewerView full bio

Dr Doug McKechnie, MRCGP
Medical Writer
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Dr Doug McKechnie is an NHS GP working in London. He works full-time clinically and is also the Deputy Lead for the Clinical and Professional Practice module at University College London Medical School.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 9 Sept 2027
10 Sept 2024 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in brain and nerves
- Alzheimer's disease
- Carpal tunnel syndrome
- Cluster headaches
- Complex regional pain syndrome (CRPS)
- Diabetic neuropathy
- Dyslexia
- Electroencephalograph
- Epilepsy and contraception
- Epilepsy medication and side-effects
- Foot drop
- Headache
- Huntington's disease
- Lumbar puncture
- Memory loss and dementia
- Migraine and combined hormonal contraception
- Neuropathic pain
- Peripheral neuropathy
- Tonic-clonic seizures
- Types of seizures
- Wilson's disease