Primary liver cancer
Peer reviewed by Dr Colin Tidy, MRCGPLast updated by Dr Toni Hazell, FRCGPLast updated 7 Aug 2023
Meets Patient’s editorial guidelines
- DownloadDownload
- Share
- Language
- Discussion
- Audio Version
- Add to preferred sources on Google
In primary liver cancer the cancer starts in the liver. In secondary liver cancer, the cancer spreads from another part of the body to the liver.
Primary liver cancer is uncommon in the UK but is common in other parts of the world. In the UK, most cases develop as a complication of scarring of the liver (cirrhosis). In general the outlook is poor. Surgery to remove the cancer is an option in a small number of cases and, if it is possible, gives the best chance of a cure.
At a glance
Primary liver cancer starts in the liver and is uncommon in the UK.
Hepatocellular carcinoma is the most common type and often develops with liver scarring (cirrhosis) or hepatitis B/C.
Early symptoms can be vague, like feeling unwell, nausea, or tiredness.
Later symptoms include tummy pain, yellow skin (jaundice), or abdominal swelling.
Treatment options include surgery, chemotherapy, and other techniques like ablation.
Regular monitoring with ultrasound and blood tests is advised for people with cirrhosis.
What is primary liver cancer?
Cancer of the liver can be divided into primary liver cancer and secondary liver cancer:
Primary liver cancer means that the cancer started in the liver. In the UK, primary liver cancer is uncommon. There are around 6,200 cases of primary liver cancer each year in the UK, making it the 18th most common cancer, accounting for 2% of all new cancer cases. It occurs most commonly in people aged 85 - 89, with 40% of all cases being diagnosed in those aged 75 or over.
Secondary (metastatic) liver cancer means that a cancer which started in another part of the body has spread to the liver. Many types of cancer can spread to the liver - most commonly, cancers of the bowel, pancreas, stomach, lung or breast. The behaviour, treatment and outlook of secondary liver cancers are often quite different to those of primary liver cancer.
The rest of this leaflet is only about primary liver cancer. In particular, it is about hepatocellular carcinoma, the most common type of primary liver cancer.
What are the types of liver cancer?
Hepatocellular carcinoma. This is the most common type. It occurs in about 9 out of 10 cases. This type of cancer originates from a liver cell (hepatocyte) which becomes cancerous. Most of the liver is made up from hepatocytes. Hepatocellular carcinoma most commonly develops as a complication of liver diseases such as scarring of the liver (cirrhosis) or hepatitis B or C.
Cholangiocarcinoma. This is uncommon. It develops from cells which line the bile duct.
Hepatoblastoma. This is a rare cancer which occurs in some young children.
Angiosarcoma. This is rare. It develops from blood vessel cells within the liver.
See the separate leaflet called Cancer for more general information about cancer.
Liver cancer symptoms
There may be no symptoms in the early stage of the disease. As the cancer grows, the first symptoms to develop may be quite vague and nonspecific. For example:
Feeling generally unwell.
Feeling sick (nausea).
Weight loss and tiredness.
Many people who develop primary liver cancer will already have symptoms associated with scarring of the liver (cirrhosis). If you already have cirrhosis and your health becomes worse quite quickly, the cause may be a liver cancer which has developed. Everyone with cirrhosis should be having regular monitoring with an ultrasound and blood tests to detect any development of a liver cancer.
As the cancer develops further, more specific symptoms which may also develop include:
Tummy (abdominal) pain over the liver area.
Yellowing (jaundice). You tend to first notice this condition when the whites of your eyes become yellow. It is due to a build-up of the chemical bilirubin which is made in the liver. This occurs if the bile duct becomes blocked by the cancer. Bile and bilirubin cannot drain out from the liver and so leak into the bloodstream.
Itch (caused by the jaundice).
Swelling of the abdomen. This can be due to the growing cancer itself. It may also be due to ascites - fluid that builds up in the abdomen - which occurs with various liver disorders.
What causes primary liver cancer?
A cancerous (malignant) tumour starts from one abnormal cell. The exact reason why a cell becomes cancerous is unclear. It is thought that something damages or alters certain genes in the cell. This makes the cell abnormal and multiply out of control.
Most people who develop a primary liver cancer have one or more of the following risk factors which seem to make liver cells more prone to becoming cancerous:
Scarring of the liver (cirrhosis)
Cirrhosis tends to progress slowly. In the UK, the common causes of cirrhosis are heavy alcohol drinking, and infection with hepatitis C. However, there are various other causes of cirrhosis. Note: most people with cirrhosis do not develop liver cancer - it occurs in only a small number of people with cirrhosis.
Long-term infection with the hepatitis B or hepatitis C virus
It typically takes 20-30 years after first becoming infected to develop primary liver cancer. Infection with these hepatitis B or hepatitis C is not common in the UK. Over the last few years, public health campaigns encouraging testing have helped to increase the number of cases of hepatitis B and C which are diagnosed and treated - hopefully this should reduce the numbers who progress to liver cancer. However, these are common infections worldwide, particularly in Asia and Africa.
Many young children in these areas are infected with the hepatitis B virus, often having caught it from their mother during pregnancy or delivery. This is why primary liver cancer is a common cancer in young adults in these areas of the world (developing 20-30 years after first being infected).
Ingesting some poisons or toxins
For example, a known risk factor is a poison called aflatoxin which contaminates some foods (for example, mouldy peanuts), mainly in developing countries. Some conditions which cause persistent inflammation of the gut increase the risk slightly of developing an uncommon type of primary liver cancer (called cholangiocarcinoma) - for example, ulcerative colitis.
Smoking
There is some evidence that smoking can increase the risk.
A parasitic infection
A parasitic infection (liver fluke) which mainly occurs in Africa and Asia increases the risk of developing a cholangiocarcinoma.
How is liver cancer diagnosed?
Screening
Screening has been recommended for people at high risk of liver cancer. This happens using ultrasound scans. Sometimes a blood test for alpha-fetoprotein (AFP) is also taken at 6- to 12-monthly intervals although this is not a very accurate test and is not routinely recommended.
These tests can detect liver cancer at an earlier stage and therefore improve the chance of successful treatment. People who might benefit from this include those with scarring of the liver (cirrhosis) associated with infection with hepatitis B or hepatitis C virus.
Initial assessment
If liver cancer is suspected, you are likely to have a number of tests. These aim to:
Confirm that you have a cancer in the liver. Also, that the cancer is a primary liver cancer and not a secondary liver cancer.
Assess the stage of the cancer. That is, how much of the liver is affected and whether the cancer has spread to other parts of the body.
Assess the state of your liver function and your general health.
Therefore, a range of tests is usually needed. Tests may include:
Scans such as an ultrasound scan, a computerised tomography (CT) scan or a magnetic resonance imaging (MRI) scan. These can help to show the exact location and extent of the cancer.
A liver biopsy. This is usually done to confirm the type of cancer. A biopsy is a procedure in which a small sample of tissue is removed from a part of the body. The sample is then examined under the microscope to look for abnormal cells.
Blood tests help to assess the liver function and your general health.
Other tests may be done if the above do not clarify the situation. For example, a laparoscopy is sometimes done. This is a small operation using a flexible telescope to look inside the tummy (abdomen).
What is the liver?
Liver function
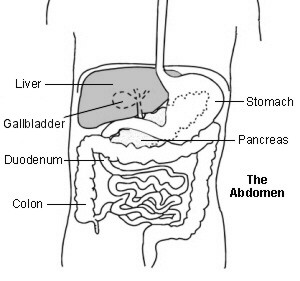
The liver is in the upper right part of the tummy (abdomen). It has many functions which include:
Storing fuel for the body (called glycogen), which is made from sugars. When required, glycogen is broken down into glucose which is released into the bloodstream.
Helping to process fats and proteins from digested food.
Making proteins that are essential for blood to clot (clotting factors).
Helping to process and/or remove alcohol, many types of medicines, toxins and poisons from the body.
Making bile which passes from the liver to the gut down the bile duct. Bile breaks down the fats in food so that they can be absorbed from the bowel.
Liver cancer treatment
The main treatments used for primary liver cancer are surgery and chemotherapy. Other techniques are sometimes used. The treatment advised in each case depends on various factors such as:
The exact site of the primary tumour in the liver.
How large the cancer is and whether it has spread (the stage of the cancer). See the separate leaflet called Stages of Cancer for more details.
Your general health. In particular, the general state of your liver and liver function. Many people with primary liver cancer also have poor liver function due to scarring of the liver (cirrhosis).
You should have a full discussion with a specialist who knows your case. They will be able to give you the pros and cons, likely success rate, the possible side-effects, and other details about the possible treatment options for your type of cancer.
You should also discuss with your specialist the aims of treatment. For example:
In some cases, treatment aims to cure the cancer. The best chance of a cure for primary liver cancer is if it is diagnosed and treated at an early stage. (Note: doctors tend to use the word 'remission' rather than 'cured'. Remission means there is no evidence of cancer following treatment. If you are in remission, you may be cured. However, in some cases a cancer returns months or years later. This is why doctors are sometimes reluctant to use the word 'cured'.)
In some cases, treatment aims to control the cancer. If a cure is not realistic, with treatment it may be possible to limit the growth or spread of the cancer so that it progresses less rapidly. This may keep you free of symptoms for some time.
In some cases, treatment aims to ease symptoms (palliative treatment). For example, if a cancer is advanced then you may require painkillers or other treatments to help keep you free of pain or other symptoms. Some treatments may be used to reduce the size of a cancer, which may ease symptoms such as pain.
Surgery
Surgery which aims to cure the cancer is an option in some cases. If the cancer is small, has not spread outside the liver and the rest of the liver is healthy, it may be possible to cut out the part of the liver which contains the cancer. Healthy liver tissue will regrow to its full size within a few weeks if a section of liver is cut out. However, this operation is not suitable if your liver is damaged with severe cirrhosis. This is often the case in many people with primary liver cancer.
A liver transplant is another option but again only suitable for a small number of cases.
Surgery also has a role in palliative care. For example, if yellowing (jaundice) is severe, it may be possible to relieve the blockage of bile by inserting a stent. This is a narrow tube which allows the bile to drain into the gut.
Another example is inserting a tube through the wall of the abdomen to drain the fluid called ascites. The fluid is produced by the damaged liver and can be very uncomfortable if a large amount builds up.
Chemotherapy
Chemotherapy is a treatment which uses anti-cancer medicines to kill cancer cells, or to stop them from multiplying. It is not likely to be curative for primary liver cancer but may shrink the tumour down to slow the progression of the disease.
There are new medicines being developed for the treatment of liver cancer. For example, sorafenib is a type of medicine called a multi-targeted kinase inhibitor. It interferes with the growth of cancer cells.
Research has shown that sorafenib can be beneficial for people with advanced hepatocellular carcinoma. National Institute for Health and Care Excellence (NICE) recommend this for the treatment of people with advanced hepatocellular carcinoma under certain conditions.
For some patients who have had sorafenib and continue to need further treatment for advanced hepatocellular carcinoma, NICE also recommends another drug called cabozantinib.
These drugs are not suitable for everyone and so you should discuss your options with your consultant.
Other treatments
Various other treatment techniques are sometimes used - for example:
Alcohol ablation. Ablation means to destroy. For this treatment, alcohol is injected into the tumour. The alcohol kills cancer cells.
Radiofrequency ablation. For this treatment, a needle is inserted into the tumour. High-intensity radio waves or laser light are then passed through the needle. This heats the cancer cells and kills them.
Cryotherapy. For this treatment, a small metal object filled with liquid nitrogen is placed into the tumour. The liquid nitrogen makes it very cold which destroys cancer cells.
Chemoembolisation. For this treatment, medicines used for chemotherapy are mixed with another oily chemical. The mixture is then injected into branches of the liver artery (hepatic artery) which are supplying the tumour with blood. The oily chemical helps to hold the chemotherapy medicines longer in the liver and make them more effective in killing cancer cells.
Radiotherapy - a treatment which uses high-energy beams of radiation which are focused on cancerous tissue. This kills cancer cells, or stops cancer cells from multiplying. Radiotherapy is not often used for primary liver cancers apart from the uncommon cholangiocarcinoma type of cancer.
What is the outlook?
Overall the outlook (prognosis) is poor. Many people who develop primary liver cancer are already in poor health with scarring of the liver (cirrhosis). The best chance of a cure is with surgery when the cancer is small, has not spread from the liver and the rest of the liver is relatively healthy. However, this situation only occurs in a small number of cases.
The various other treatments described above may delay the progression of the disease but often will not cure it. More information on treatment and staging can be found in the EASL Guideline in 'Further Reading' below.
The treatment of cancer is a developing area of medicine. New treatments continue to be developed and the information on outlook above is very general. The specialist who knows your case can give more accurate information about your particular outlook, and how well your type and stage of cancer are likely to respond to treatment.
How to prevent liver cancer
Primary liver cancer can be prevented with vaccination against hepatitis B. Vaccination against hepatitis B is recommended by the World Health Organization for all newborns and high-risk groups. Vaccination is also recommended for young adolescents and people at higher risk of exposure to hepatitis B, such as health workers, travellers to areas where hepatitis B is common, injecting drug users, and people with multiple sex partners.
Avoiding excessive alcohol use is also important, as cirrhosis is more common in those who drink heavily and cirrhosis can progress to liver cancer. The current UK recommendation is that both men and women drink no more than 14 units of alcohol per week, spread across at least three days of the week.
In patients with chronic hepatitis B or C, antiviral therapies are recommended, since there is very good evidence that they prevent progression to cirrhosis and possible development of liver cancer.
When someone has already developed cirrhosis, antiviral therapy is still beneficial as it prevents cirrhosis worsening and possible liver failure. Note: successful antiviral therapy reduces but does not remove the risk of liver cancer developing.
Coffee consumption has been shown to lower the risk of primary liver cancer in patients with chronic liver disease. In these patients, coffee consumption should be encouraged.
Patient picks for Gastrointestinal cancers

Cancer
Oesophageal cancer
Oesophageal cancer is cancer of the gullet (oesophagus). There are over 8,000 new cases diagnosed every year in the UK and two thirds of new diagnoses are in men.t is the 7th most common cause of cancer death in the UK and accounts for 5% of all cancer deaths. Most cases occur in people over the age of 55, although younger people are sometimes affected. Those diagnosed at an early stage have the best chance of a cure. The earliest symptom is often difficulty with swallowing (dysphagia).
by Dr Toni Hazell, FRCGP

Cancer
Stomach cancer
Although stomach (gastric) cancer is common worldwide, it is not so common in the UK. Most cases occur in people over the age of 55. If stomach cancer is diagnosed at an early stage, there is a good chance of a cure. In general, the more advanced the cancer (the more it has grown and spread), the less chance that treatment will be curative. However, treatment can often slow the progress of the cancer.
by Dr Doug McKechnie, MRCGP
Frequently asked questions
What is the likelihood of developing liver cancer if I have cirrhosis?
While cirrhosis is a significant risk factor for primary liver cancer, most people with cirrhosis do not develop it. It only occurs in a small number of individuals with the condition.
Are there different kinds of primary liver cancer?
Yes, there are several types of primary liver cancer. The most common is hepatocellular carcinoma, which makes up about 9 out of 10 cases and starts from liver cells. Other rarer types include cholangiocarcinoma, which develops from cells lining the bile duct; hepatoblastoma, seen in some young children; and angiosarcoma, which forms in the liver's blood vessel cells.
How accurate are screening tests for liver cancer?
Screening for liver cancer in high-risk individuals often involves ultrasound scans, which can help detect cancer at an earlier stage and improve treatment success. A blood test for alpha-fetoprotein (AFP) is sometimes used but is not considered very accurate and isn't routinely recommended.
What is the difference between remission and being cured of liver cancer?
Doctors typically use the word 'remission' rather than 'cured' because remission means there is no evidence of cancer after treatment. While you might be cured, some cancers can return months or years later, which is why medical professionals are often hesitant to use the term 'cured.' Treatment aims can include curing the cancer, controlling its growth, or easing symptoms.
What role does coffee play in preventing liver cancer?
For patients who have chronic liver disease, coffee consumption has been shown to potentially lower the risk of primary liver cancer. Therefore, in these cases, coffee consumption is encouraged.
Further reading and references
- Microwave ablation of hepatocellular carcinoma; NICE Interventional Procedure Guidance, March 2007
- Forner A, Llovet JM, Bruix J; Hepatocellular carcinoma. Lancet. 2012 Mar 31;379(9822):1245-55. Epub 2012 Feb 20.
- Liver cancer statistics; Cancer Research UK
- Salhab M, Canelo R; An overview of evidence-based management of hepatocellular carcinoma: a meta-analysis. J Cancer Res Ther. 2011 Oct-Dec;7(4):463-75.
- Cirrhosis in over 16s - assessment and management; NICE Guideline (July 2016 - last updated September 2023)
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma; European Association for the Study of the Liver (2018)
- Cabozantinib for previously treated advanced hepatocellular carcinoma; NICE Technology appraisal guidance, December 2022
- Sorafenib for treating advanced hepatocellular carcinoma; NICE Technology Appraisal Guidance [TA474], September 2017.
About the authorView full bio

Dr Toni Hazell, FRCGP
MBBS, BSc, FRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
General Practitioner, Medical Author
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Article history
The information on this page is written and peer reviewed by qualified clinicians.
Article also available in English, German, Spanish, French, Italian, Portuguese, Hindi, Hebrew, Arabic, and Swedish.
Next review due: 5 Aug 2028
7 Aug 2023 | Latest version

Ask, share, connect.
Browse discussions, ask questions, and share experiences across hundreds of health topics.

Feeling unwell?
Assess your symptoms online for free
Sign up to the Patient newsletter
Your weekly dose of clear, trustworthy health advice - written to help you feel informed, confident and in control.
By subscribing you accept our Privacy Policy. You can unsubscribe at any time. We never sell your data.
More in cancer
- Acute myeloid leukaemia
- Bone marrow biopsy and aspiration
- Breast cancer facts and risk factors
- Breast screening
- Cervical cancer
- Chronic lymphocytic leukaemia
- Lung cancer
- Mouth cancer
- Mucositis
- Neuroblastoma
- Oesophageal cancer
- Prostate cancer
- Radiotherapy
- Rhabdomyosarcoma
- Skin cancer types
- Stages of cancer
- Stomach cancer
- Types of cancer
- Wilms' tumour